1Department of Kayachikitsa, All India Institute of Ayurveda, Mathura Road, New Delhi, INDIA
2Department of RNVV, FIMS, SGT University, Budhera, Gurugram, Haryana, INDIA
3Research Advisor, All India Institute of Ayurveda, Mathura Road, New Delhi, INDIA
Corresponding author.
Author Notes
ABSTRACT
Background
With a high incidence and prevalence of Diabetes and an increase in population of elderly, reports project the number of diagnosed diabetes cases among people 65 years and older will grow more than 4-fold from 2005 to 2050. Diabetes has been identified as a potential risk factor requiring hospitalisation for SARS-CoV-2, Due to mechanisms like chronic inflammation, impaired immune response, etc. Madhumeha (Diabetes) is a condition with depletion of Ojus. Thus, Rasayana Chikitsa is an imperative requirement to manage the disease and to prevent the complications. Increased awareness amongst large population groups should be a major determinant for the prevention of diabetes and its complications. Therefore, Knowledge, Attitude, and Practice were chosen to study as the principal markers of awareness among patients.
Materials and Methods
An cross sectional pilot study was planned to assess the Knowledge, Attitude and Practices related to Rasayana Chikitsa among Elderly Diabetic subjects during the COVID 19 Pandemic. Non-probable convenient sampling was done to enroll 50 subjects, by using an interviewer-based questionnaire.
Results
Gender, Educational status and socioeconomic status were strong positive indicators of Knowledge and practice. Females had better Knowledge (16.10 vs 10.9), Attitude (6.9 vs 6) and Practice (5.4 vs 3.2) scores compared to males. One in two respondents knew about Ayurvedic immunomodulators (50%) and 64% of them came to know it during the pandemic, but nearly half (46% responded “Don’t know”) did not have a definite positive attitude that Ayurvedic immunomodulators would control the infection.
Conclusion
Even though there is good knowledge about the disease and moderate knowledge about the Rasayana Chikitsa, there is a considerable gap when it comes to practice. Hence, there is an urgent need for coordinated educational campaigns with a prioritized focus on poorer, rural and less educated groups to combat negative attitude and poor practices about uses of Ayurvedic immunomodulators.
INTRODUCTION
According to the World Health Organization (WHO), viral diseases continue to emerge and represent a serious issue to public health. In the last twenty years, several viral epidemics such as the severe acute respiratory syndrome coronavirus (SARS-CoV) in 2002 to 2003, and H1N1 influenza in 2009, have been recorded.
In a timeline that reaches the present day, an epidemic of cases with unexplained low respiratory infections detected in Wuhan was first reported to the WHO Country Office in China, on December 31, 2019. Published literature can trace the beginning of symptomatic individuals back to the beginning of December 2019. As they were unable to identify the causative agent, these first cases classified as “pneumonia of unknown aetiology” and later declared as COVID-19.1
COVID-19 and comorbidities
It has been observed that most severe and fatal cases with COVID-19 have occurred in the elderly or in patients with underlying comorbidities, particularly Cerebro-Vascular Diseases (CVD), Diabetes Mellitus (DM), chronic lung and renal disease, Hypertension, and Cancer. One Chinese meta-analysis including 1527 patients showed that Diabetes Mellitus was the third most prevalent metabolic comorbidity with COVID-19 (9.7%, 95% C:I 6.9-12.5). In this report, patients with diabetes had a 2-fold increase in risk of severe disease or requiring Intensive Care Unit admission.2
Association between COVID-19, Diabetes and Immunity
Infections, particularly influenza and pneumonia, are often common and more serious in older people with Type 2 Diabetes Mellitus (T2DM). Diabetes and uncontrolled glycaemia were reported as significant predictors of severity and deaths in patients infected with different viruses, including the 2009 pandemic influenza A (H1N1), SARS-CoV and MERS-CoV.3
Infection of SARS-CoV-2 in those with diabetes possibly triggers higher stress conditions, with greater release of hyperglycemic hormones, e.g., glucocorticoids and catecholamines, leading to increased blood glucose levels and abnormal glucose variability. Hyperglycemia and insulin resistance promote increased synthesis of glycosylation end products (AGEs) and pro-inflammatory cytokines etc. Chronic inflammation, increased coagulation activity, immune response impairment, and potential direct pancreatic damage by SARS-CoV-2 might be among the underlying mechanisms of the association between diabetes and COVID-19.2
In vitro studies have shown that exposure of pulmonary epithelial cells to high glucose concentrations significantly increases influenza virus infection and replication, indicating that hyperglycemia may enhance viral replication in vivo.4
The International Diabetes Federation has estimated in 2015 that, globally there are 415 million people had Diabetes and predicted to increase to 642 million by 2040. In the world, India stands second, with 69.2 million people having diagnosed with Diabetes and another 36.5 million with prediabetes which is a high-risk condition for both DM and CVD. The Cost of Diabetes management in India (CODI) was a large community-based survey related to patient expenditure made on management of Diabetes. According to this study, ambulatory care constitutes 65% of the total cost whereas hospitalization accounts for 35%. This expenditure can be considerably reduced by increasing the awareness about complications and self-care.5
Old age by itself is risk factor for many of the diseases and its complications and is in jeopardy for increased morbidity. As explained, diseases occurring at young ages (yunah/taruna state of body) is said to be easily curable, but the opposite is not true i.e. diseases in elderly age group is difficult to cure or incurable.6
India is in a phase of demographic transition. As per the 1991 census, the population of the elderly in India was 57 million as compared with 20 million in 1951. There has been a sharp increase in the number of elderly persons between 1991 and 2001 and it has been projected that by the year 2050, the number of elderly people would rise to about 324 million. India may soon acquire the label of “an ageing nation” with 7.7% of its population being older than 60 years.7
In general, 20% of old people have DM, and similar proportions have undiagnosed DM. Reported frequencies vary from 18% to 33%. This range may reflect differences in the age, life style, and genetic background of the analysed populations. On another hand, 30% of old people have impaired glucose regulation which means an increased risk for DM.8,9
In India, nearly 5.8 million people (WHO report, 2015) die from NCDs (heart and lung diseases, stroke, cancer and diabetes) every year or in other words 1 in 4 Indians has a risk of dying from an NCD before they reach the age of 70. It is found that there is increase in the contribution of NCDs from 30% of the total disease burden- ‘Disability-Adjusted Life Years’ (DALYs) in 1990 to 55% in 2016 and also an increase in proportion of deaths due to NCDs (among all deaths) from 37% in 1990 to 61% in 2016.10 Many national health schemes are addressing this cause effectively.
Global herbal medicine market is expected to exceed 411 billion USD by 2026. Ayurveda contributes to almost 7.5% of this market share. At this juncture it becomes the solitary responsibility of Ayurveda intellectuals to provide authentic Evidenced based knowledge to the society which would be helpful to create awareness among scientific community and common public.11
The burden of diabetes on health of the society continues to grow. With an increase in the incidence of Diabetes and population of elderly, the proportion of elderly patients with diabetes will continue to rise. The risk of Diabetes is also increasing in the middle-aged population and thus demand medical services for a prolonged duration of disease. Diabetes increases the risk of falls, urinary incontinence, dementia, depression and vision and hearing loss in elderly.
It is extensively being realized that many of the NCDs occur due to “oxidative stress” that results from an imbalance between formation and neutralization of free radicals, finally leading to impaired immunity. And in such cases regular consumption of antioxidants and immunomodulators are highly recommended. A wide variety of Pharmacological and Non pharmacological modalities are explained under Rasayana chikitsa, including Curative, Preventive, Cognitive-fostering, Attribute-enhancing etc. Main purpose of Rasayana chikitsa is to maintain excellency of body tissues, delay the onset of senility, increase longevity, prevent the adversities of disease and old age. Madhumeha is a disease of hampered Ojus (~Immunity), demanding the specific usage of curative and promotive Rasayana. As per the texts of Ayurveda, a physician’s role is to just aid the cure of an ailment and most of the health restoration is done by one’s own body. This foregrounds the importance of Knowledge about diseases and self-care practices.
Pandemic time has exponentially increased the digital literacy and easier access to information. In general, it seems that awareness about Ayurvedic therapies have increased among the public in COVID-19 pandemic era. In order to study this scenario systematically, this pilot study was planned for the assessment of Knowledge, Attitude and Practice regarding Rasayana chikitsa (Ayurvedic Immunomodulators) in elderly Diabetic population, which could facilitate targeted screening and prevention efforts among this vulnerable population.
Objectives
The objective of this study was to check the demographic profile of patients with T2DM attending the Ayurvedic OPD. This study was carried out to determine Knowledge, Attitude, Practices and their predictors, regarding Ayurvedic RASAYANA THERAPY among elderly Diabetic patients attending an Ayurvedic Tertiary Care hospital in Delhi, during the Pandemic era.
MATERIALS AND METHODS
Study design and area
An cross sectional pilot study was carried out for the assessment. Patients were recruited from the Outpatient department of Kayachikitsa, attending the Diabetes and metabolic disorders OPD of the All India Institute of Ayurveda, New Delhi. Hospital is a Tertiary Care Centre established in an urban setting.
Target population and study size
All Patients diagnosed with Type 2 Diabetes Mellitus and aged older than 60 years on their 1st visit were included. Recruitment was done from September 2020 to January 2021 from the outpatient department. Those not willing to answer or unable to answer the questionnaire because of age related cognitive disabilities like dementia, etc were excluded from the study. Among all the suitable subjects, a total of 50 subjects were included for this pilot study.
Data collection tool and approach
Non-probable convenient sampling was done to enroll; the subjects. A structured questionnaire was prepared by reviewing studies on similar subject. The questionnaire had two sections, Part 1 with Demographic details, Part 2 comprising of close-ended questions to assess Knowledge (20 Questions), Attitude (12 Questions) and Practices (11 Questions). Questions under all the three subsections were framed to evaluate Knowledge, Attitude, Practice regarding the diagnosed disease, its Ayurvedic counterpart, and Ayurvedic medicine in general, and Rasayana therapy in specific. Answers to the Knowledge and Practice questions were dichotomized (Yes/No). Responses to the item evaluating attitudes toward DM and its treatment were also categorical (Yes/No/Don’t know). Knowledge questions were reclassified based on components to be assessed. Among 20 questions, four questions assessed knowledge regarding Nidana (~Aetiology), four assessed Upashaya-Anupashaya, two assessed knowledge regarding COVID-19, four about Ayurveda chikitsa including Rasayana, and remaining six about general disease knowledge. It was an interviewer-based questionnaire and was conducted face-to-face by a single interviewer who was aware of survey objectives and interview principles. Medical records were inspected to access recent Fasting Blood Sugar levels (within last 3 months), retrospectively. Ethical considerations were taken care off by taking verbal consent and maintaining the confidentiality.
Outcome measures
The primary outcome measures were Knowledge, Attitude and Practice scores. The secondary outcome measure was the predictors of knowledge, attitude and practice.
Operational definition
To calculate KAP score, a scoring system was prepared. Each agreement with the positive component of the item would have one score added while each incorrect answer was given with 0. Positive response to each known complication was also given with a positive one score. Response of “Don’t know” was also given a score of 0 under attitude section. While this did allow for direct comparison along the continuum of positive versus negative attitude. Score grading regarding the KAP is given in Table 1.
| Sl. No. | Sub-section | Scoring | % of N |
|---|---|---|---|
| 1 | Knowledge | Mild 0 – 12 | 28 |
| Moderate 13-25 | 64 | ||
| High 26-37 | 8 | ||
| 2 | Attitude | Mild 0-4 | 6 |
| Moderate 5-9 | 74 | ||
| High 10-12 | 20 | ||
| 3 | Practice | Mild 0-3 | 28 |
| Moderate 4-7 | 46 | ||
| High 8-11 | 26 |
Knowledge Attitude Practice distribution among study participants.
Data analysis method
The collected data was entered in the Statistics Package for Social Science (SPSS) version 26 for Windows. All continuous data were expressed as mean, median and Standard Deviations and categorical variables were expressed as numbers and percentages. Descriptive statistics and frequency distributions were used to describe participant characteristics. The respondent’s socioeconomic status was calculated using Kuppuswamy Scale.12 Chi-square test, Pearson Correlation; Fisher’s exact tests were used at appropriate stages. p values of 0.05 was considered significant and 95% confidence interval computed. For cross analysis, Knowledge was considered as an independent variable. For attitude analysis, Knowledge was considered and for practice analysis both knowledge and attitude score were considered with the help of Cross tabulation and Pearsons correlation and Multiple Logistic Regression.
RESULTS
Demographic details
Demographic characteristics of the respondents are summarised in Table 2. Average age of the respondents was 62.9 years. It was found that patients attending OPD were consuming the Ayurvedic medications on an average for 24.4 months, with an average history of DM of 10.4 years. Respondents were observed to have moderate control of Blood Sugar Level (BSL) (FBS-170.2 mg/dL).
| Sl. No. | Background characteristics | Category | Percentage |
|---|---|---|---|
| 1 | Educational qualification | Illiterate | 16 |
| Primary | 12 | ||
| Secondary | 26 | ||
| Pre university | 18 | ||
| Graduate | 20 | ||
| Post graduate and PhD | 8 | ||
| 2 | Gender | Male | 62 |
| Female | 38 | ||
| 3 | Socio-economic status | Upper class | 12 |
| Upper middle class | 24 | ||
| Lower middle class | 56 | ||
| Upper lower class | 4 | ||
| Lower class | 4 | ||
| 4 | Occupation | Employed | 70 |
| Unemployed | 30 | ||
| 5 | Source of introduction to Ayurveda | Neighbour | 40 |
| Relative | 32 | ||
| Self | 28 |
Demographic characteristics of study sample.
Knowledge, Attitude and Practice scores
Knowledge
Overall Knowledge score was 16.9/37 (SD-7.5, MIN-3, MAX-31, Median-19). 58% of the respondents were aware that Madhumeha is a hereditary disorder. Most number of respondents (92%) knew the harmful effects of Sweet and Dairy products on BSL. 74% and 78% of the sample knew atleast one complication and sign of Diabetes respectively. Details are given in Figure 1a and 1b. Knowledge about the rules of taking Oral Hypoglycaemic Agents (OHA) (48%) was better than knowledge of effects of regular physical exercise (24%). However, least knowledge was regarding the importance and effects of Ayurvedic Rasayana (Immunomodulators) (20%) followed by effects of Physical exercise (24%), and mental stress on BSL (40%). 52% of them were aware that being elderly, they are more prone to get infected and can have a more severe disease by COVID-19. One in two respondents knew about Ayurvedic immunomodulators (50%) and 64% of them came to know it during the pandemic.

Figure 1a:
Knowledge of Complications of Madumeha.
Figure 1b:
Knowledge of Symptoms of Madhumeha.
Attitude
Overall Attitude score was 8/12 (SD-2.20, MIN-3, MAX-12, Median-8). 80% of the subjects believed that intake of controlled diet would help control BSL. 92% of them had a positive attitude towards Ayurvedic medicine regarding management of Diabetes. Majority of them (96%) believed Ayurvedic medicine has less complications compared to conventional medicine. 50% of the respondents were not certain about who is responsible (Doctor/ Family/Self) for the control of their diseased condition. Only 32% were positive about their active role in controlling the disease. Nearly half of them (48%) believed drug is more important than diet to control the disease. 86% of the subjects had a negative attitude about the Ayurvedic treatment, reasoning to the strict dietic regimens and rules. And one in two individuals would think to avoid it for the same reason. 68% of them believed, community had more awareness about Ayurvedic immunomodulators after COVID-19 pandemic, but nearly half (46% responded “Don’t know”) did not have a definite positive attitude that Ayurvedic immunomodulators would control the infection.
Practice
Overall practice score was 5.4/11 (SD-2.7, MIN-0, MAX-11, Median-5.5). Only 30% of them practiced physical exercise for more than 40 mins a day. 56% of the subjects regularly checked their BSL, even though 64% of them had their own Glucometer. Among all the 50 enrolled subjects, only 82% took regular Ayurvedic medicines for Madhumeha. 26% of them attended atleast one patient education program regarding their diseased condition in last 6 months. 44% practised regular homebased Ayurvedic regimens like Golden milk intake, oil massage, Intake of avla, haldi etc. and 80% of these subjects started it after the pandemic. Percentage of population with mild, moderate, and high KAP score is described in Table 1.
DISCUSSION
Demographics and its influence on KAP score
Though there are number of KAP studies reported at a Tertiary Care hospital in Delhi NCR among patients of Diabetes Mellitus, this cross-sectional study is the first known study being reported on the Knowledge Attitude and Practice of Ayurvedic Rasayana therapies among patients attending OPD at an Ayurveda Tertiary Care hospital. As the study was carried out in an urban setup, it reveals that 20% were graduates and 26% Secondary school educated and majority of respondents from Lower middle class (56%) in this study. Only 30% of the subjects visited a Specialist/Endocrinologist which might be because of issues with affordability or accessibility. Both affordability and literacy may be a problem in diabetes education and management.13,14 Most of respondents were introduced to Ayurveda medicine by their neighbours. This emphasises the positive role of community interactions on awareness of Ayurveda. By the percentage of positive responses to questions related to Ayurvedic regimes, it is evident that pandemic has increased the KAP among population.
Due to social media influence and digitally accessible medical care, it has made the population to know more and understand better about the Ayurvedic therapies.15 This digital competence also comes with a disadvantage of circulation of insufficient and defective knowledge.16 Hence, it becomes the responsibility of the authority of Ayurveda systems of medicine, to ensure the circulation and availability of authentic knowledge. Lack of certainty regarding the responsible role of oneself in controlling disease shows a huge deficit in motivation, patient education and implementation of health missions. It has been proven that self-care significantly improved the glycaemic control.17,18 Indefinite responses to the question assessing the superiority among Drug and Diet in the management of Diabetes, accentuates the need of propagating the core principles of Ayurveda such as Pathya. Negative responses to questions assessing the attitude towards dietetic restriction and avoidance of treatment for the same, highlights the false believes among people about dietary and activity restriction and proper patient education is the only solution out for this.19
Relation between duration of Ayurvedic medicine intake and KAP
It was found that duration of Ayurveda medicine intake had high correlation when it comes to Knowledge and Attitude of the Immunomodulators. Details are given in Table 3. As the duration increased, percentage of positive response increased and percentage of unsure response decreased. There was no relation found between level of BSL and knowledge, attitude and practice scores. Gender, Educational status and socioeconomic status were strong positive indicators of Knowledge and practice. Females had better Knowledge scores (16.1 vs 10.9), Attitude (6.9 vs 6) and Practice (5.4 vs 3.2) compared to males. These findings are consistent with other studies too.20–22 Chronicity of the disease significantly increased the Knowledge (p<0.01) and Practice score (p<0.01). Chronicity of the disease also increased the knowledge of complications as depicted in Table 4. 74% of them knew atleast one complication, a finding which is in contrary to other studies from Bangladesh (51.1%) and Iran (59.6%) respectively.23,24 In this study, almost 68% respondents knew the harmful effects of smoking and alcohol on BSL in comparison nearly half of the respondents were unaware of its ill effects.24 Patient compliance to Ayurvedic medication among the respondents attending the OPD was 82% and not 100% as expected. This emphasises the need of patient motivation and education about adherence and obedience to physician advice among the public, including the ones attending an Ayurvedic health centre.
| Sl. No. | Question | Duration | Percentage of Positive response | Percentage of unsure response |
|---|---|---|---|---|
| 1 | K16 – Do you know about special treatment for elderly in Ayurveda? | <1 year | 38.7 | NA |
| >1 year | 57.9 | NA | ||
| 2 | K17-Do you know about Rasayana? | <1 year | 38.7 | NA |
| >1 year | 68.4 | NA | ||
| 3 | K19-Do you know about Panchakarma treatments done in Madhumeha? | <1 year | 45.2 | NA |
| >1 year | 68.4 | NA | ||
| 4 | K20 -Do you the importance of Avla, Haldi etc as Rasayana? | <1 year | 12.9 | NA |
| >1 year | 31.6 | NA | ||
| 5 | A11 – Do you believe taking Ayurvedic Rasayana drugs would help in controlling infectious diseases like COVID-19? | <1 year | 41.9 | 51.6 |
| >1 year | 63.2 | 36.8 | ||
| 6 | A12 – Do you think pandemic has increased the awareness about Ayurvedic immunomodulators among common public? | <1 year | 61.3 | 38.7 |
| >1 year | 78.9 | 21.1 | ||
| 7 | P7 – Do you attend any educational/ awareness programs related to Ayurveda? | <1 year | 22.6 | NA |
| >1 year | 31.6 | NA | ||
| 8 | P8 – Being elderly Diabetic, do you follow any Ayurvedic habits/regimens regularly? | <1 year | 22.6 | NA |
| >1 year | 78.9 | NA |
Relation between duration of Ayurveda medicine intake and KAP.
| Sl. No. | Complication | Chronicity of Disease | Percentage of subjects knowing the complication | Percentage of subjects not knowing the complication |
|---|---|---|---|---|
| 1 | Foot problem | Less than 5 years | 0 | 100 |
| 5-10 years | 0 | 100 | ||
| More than 10 years | 26 | 74 | ||
| 2 | Kidney disease | Less than 5 years | 23 | 77 |
| 5-10 years | 80 | 20 | ||
| More than 10 years | 91 | 8 | ||
| 3 | Hypertension | Less than 5 years | 0 | 100 |
| 5-10 years | 0 | 100 | ||
| More than 10 years | 21 | 79 | ||
| 4 | Herat attack | Less than 5 years | 23 | 77 |
| 5-10 years | 60 | 40 | ||
| More than 10 years | 61 | 39 | ||
| 5 | Stroke | Less than 5 years | 0 | 100 |
| 5-10 years | 0 | 100 | ||
| More than 10 years | 17 | 83 | ||
| 6 | Eye disease | Less than 5 years | 24 | 76 |
| 5-10 years | 100 | 0 | ||
| More than 10 years | 74 | 26 | ||
| 7 | Teeth and gum disease | Less than 5 years | 0 | 100 |
| 5-10 years | 20 | 80 | ||
| More than 10 years | 17 | 83 | ||
| 8 | Sexual dysfunction | Less than 5 years | 0 | 100 |
| 5-10 years | 0 | 100 | ||
| More than 10 years | 9 | 91 |
Chronicity and knowledge of complications.
Correlation between Knowledge, Attitude and Practice score
A total of 44% of the respondents with upto median Knowledge score had above median attitude and 48% of respondents with above median knowledge score had above median attitude score. Even though there was a positive correlation between knowledge and attitude, it was not significant. 18% of the respondents with upto median Knowledge score had above median Practice and 72% of respondents with above median knowledge score had above median practice score. This showed a significant positive correlation between Knowledge and Practice (p=0.002). 66.7% of the respondents with upto median Attitude score had above median Practice and 30.4% of respondents with above median attitude score had above median practice score. There was a significant negative correlation between and attitude and practice (p=0.011). This observation might have been because of a greater number of respondents answering “Don’t know” compared to “Disagree” response under Attitude questions. This extensively reveals the lack of presence of authentic knowledge regarding Ayurvedic therapies and immunomodulators in the community leading to uncertain and speculative responses. Correlation between Knowledge, Attitude and Practice has been summarized in Figure 2.
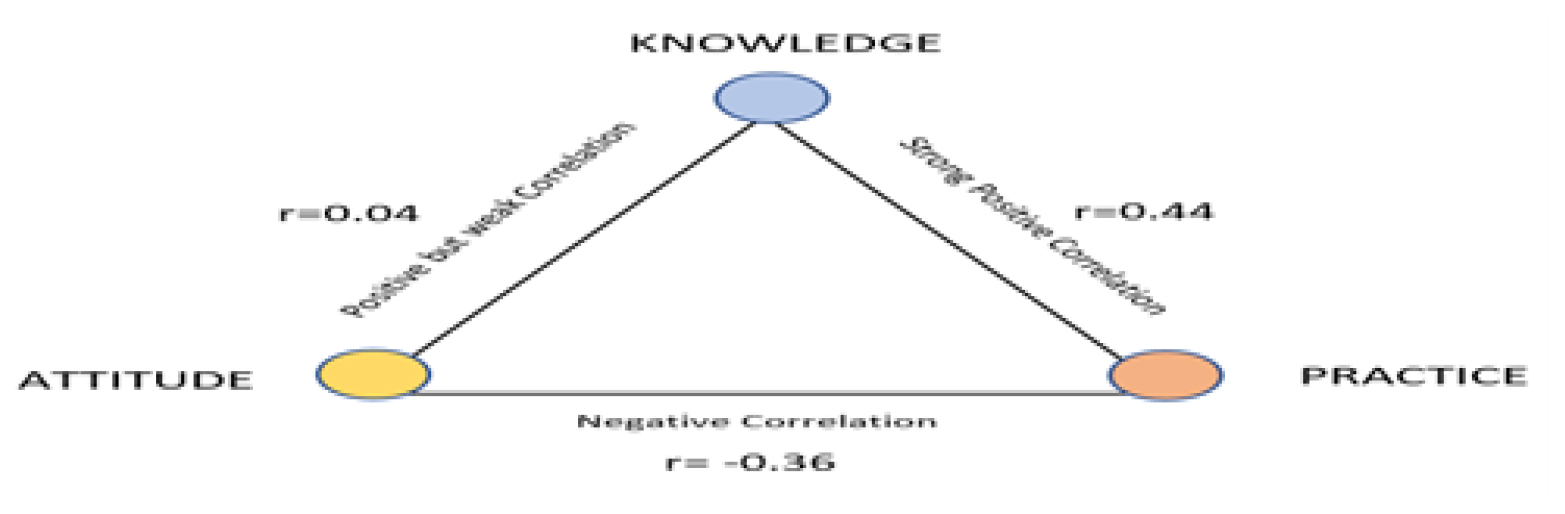
Figure 2:
Summary of Pearson Correlation (r).
Patient education is the most constructive track that could assist with early detection, lessen complication and assist management of diabetes.25-27 Reaching out to the diseased population at a healthcare facility is superior, convenient and less time consuming when compared to addressing the population in a community setup. Therefore, Ayurvedic hospitals should take up and map out a greater number of patient awareness initiatives at their setting which would aid in providing a realistic and more effective awareness and guidance.
CONCLUSION
Moderate knowledge, moderate positive attitude, and poor practice level were found in this surveyed community, particularly in males, illiterates and low-income groups. Recently diagnosed cases, and young aged people need greater attention in educational campaigns and physicians counselling so as to get a better and quick outcome. Physician’s and healthcare centre’s active participation and time for providing structured education and counselling about authentic and published materials regarding Ayurvedic therapies and Immunomodulators may bring better therapeutic outcome and lessen complications. Self-management should be encouraged and role of self in preventing the complications should be sensitized. Source of information collected in this study will help identify popular patient community that should be strengthened for future awareness and provide an educational base for patients. Ayurvedic hospitals can engage patients through practical and enjoyable methods such as kitchen garden teaching classes, culinary medicine sessions, and health challenges. These initiatives resonate deeply with patients, fostering a sense of connection and motivation to actively participate in their wellness journey. COVID-19 pandemic gave a tremendous boost for the practice of traditional medicines worldwide. Due to increasing digital literacy, it also led to increased cognizance among public. Taking this opportunity forward, it becomes the solitary responsibility of Ayurveda scholars to expand the base of available authentic knowledge and practice among population, and reinforce the entire Ayurveda medicinal system with multitudinous fresh windows in future.
Cite this article
Mythri HS, Krishnan NR, Mahto RR, Kumar A. Knowledge, Attitude, and Practices about Ayurvedic Immunomodulators among Elderly Diabetic Population during the COVID-19 Pandemic-A Cross-Sectional Pilot Study. Int. J. Pharm. Investigation. 2024;14(2):568-76.
ACKNOWLEDGEMENT
The authors would like to acknowledge all the participants involved in the study for cooperation and time in participating in the study.
ABBREVIATIONS
| WHO | World Health Organization |
|---|---|
| SARS-CoV | Severe Acute Respiratory Syndrome coronavirus |
| CVD | Cerebro-Vascular Diseases |
| DM | Diabetes Mellitus |
| CODI | Cost of Diabetes management in India |
| AGE | Advanced Glycation End products |
| DALY | Disability-Adjusted Life Years |
| NCD | Non Communicable Diseases |
| BSL | Blood Sugar Level |
| FBS | Fasting Blood Sugar |
| OHA | Oral Hypoglycaemic Agents |
| SD | Standard Deviation |
References
- Cascella M, Rajnik M, Cuomo A, Dulebohn SC, Di Napoli R. NCBI. Features, evaluation and treatment coronavirus (COVID-19). StatPearls [internet]. [Google Scholar]

- Hussain A, Bhowmik B, do Vale Moreira NC. COVID-19 and diabetes: knowledge in progress. Diabetes Res Clin Pract. 2020;162:108142 [PubMed] | [CrossRef] | [Google Scholar]
- Gupta R, Ghosh A, Singh AK, Anoop Misraa c. Clinical considerations for patients with diabetes in times of COVID-19 epidemic. Diabetes Metab Syndr. 2020;14(3):211-2. Published online 2020 [PubMed] | [CrossRef] | [Google Scholar]
- Hulme KD, Gallo LA, Short KR. Influenza virus and glycemic variability in diabetes: A killer combination?. Front Microbiol. 2017;8:861 [PubMed] | [CrossRef] | [Google Scholar]
- Available fromhttps://www.nhp.gov.in/overview-of-diabetes-burden_mtl.Lad; 2021
- . 1/33 page;20, published by Chaukambha Suranharathi Prakashana. [PubMed] | [CrossRef] | [Google Scholar]
- Ingle GK, Nath A. Indian J Community Med. Geriatric health in India: concerns and solutions. 2008;33(4):214-8. [PubMed] | [CrossRef] | [Google Scholar]
- Chentli F, Azzoug S, Mahgoun S. Indian J Endocrinol Metab. Diabetes mellitus in elderly. 2015;19(6):744-52. [PubMed] | [CrossRef] | [Google Scholar]
- Array. 2013;13(6)
https://www.wbhealth.gov.in/NCD/.LAD-2021 - Available fromhttps://www.medicalbuyer.co.in/herbal-medicine-market-size-worth-usd-411-2-billion-by-2026-cagr-20-5/.Lad;2021
- Wani RT. Socioeconomic status scales-modified Kuppuswamy and Udai Pareekh’s scale updated for 2019. J Fam Med Prim Care. 2019;8(6):1846-9. [PubMed] | [CrossRef] | [Google Scholar]
- Flatz A, Casillas A, Stringhini S, Zuercher E, Burnand B, Peytremann-Bridevaux I, et al. Association between education and quality of diabetes care in Switzerland. Int J Gen Med. 2015;8:87-92. Published online [PubMed] | [CrossRef] | [Google Scholar]
- Al-Rasheedi AAS. The role of educational level in glycemic control among patients with type II diabetes mellitus. Int J Health Sci (Qassim). 2014;8(2):177-87. [PubMed] | [CrossRef] | [Google Scholar]
- Patil U, Kostareva U, Hadley M, Manganello JA, Okan O, Dadaczynski K, et al. Health literacy, digital health literacy, and COVID-19 pandemic attitudes and behaviors in U.S. College students: implications for interventions. Int J Environ Res Public Health. 2021;18(6) [PubMed] | [CrossRef] | [Google Scholar]
- Gabarron E, Oyeyemi SO, Wynn R. COVID-19-related misinformation on social media: a systematic review. Bull World Health Organ. 2021;99(6):455-463A. [PubMed] | [CrossRef] | [Google Scholar]
- Shrivastava SR, Shrivastava PS, Ramasamy J. Role of self-care in management of diabetes mellitus. J Diabetes Metab Disord. 2013;12(1):14 [PubMed] | [CrossRef] | [Google Scholar]
- Rajasekharan D, Kulkarni V, Unnikrishnan B, Kumar N, Holla R, Thapar R, et al. Self-care activities among patients with diabetes attending a tertiary Care Hospital in Mangalore Karnataka, India. Ann Med Health Sci Res. 2015;5(1):59-64. [PubMed] | [CrossRef] | [Google Scholar]
- Memon MS, Shaikh SA, Shaikh AR, Fahim MF, N Mumtaz S, Ahmed N, et al. An assessment of knowledge, attitude and practices (KAP) towards diabetes and diabetic retinopathy in a suburban town of Karachi. Pak J Med Sci. 2015;31(1):183-8. [PubMed] | [CrossRef] | [Google Scholar]
- Rahaman KS, Majdzadeh R, Holakouie Naieni K, Raza O. Knowledge, attitude and practices (KAP) regarding chronic complications of diabetes among patients with Type 2 diabetes in Dhaka. Int J Endocrinol Metab. 2017;15(3):e12555 [PubMed] | [CrossRef] | [Google Scholar]
- Feleke SA. Assessment of the level and associated Factorswith knowledge and practice of diabetes mellitus among diabetic patients attending at FelegeHiwot hospital, Northwest Ethiopia. Clin Med Res. 2013;2(6):110 [CrossRef] | [Google Scholar]
- Shah VN, Kamdar PK, Shah N. Assessing the knowledge, attitudes and practice of type 2 diabetes among patients of Saurashtra region, Gujarat. Int J Diabetes Dev Ctries. 2009;29(3):118-22. [PubMed] | [CrossRef] | [Google Scholar]
- Saleh F, Mumu SJ, Ara F, Begum HA, Ali L. Knowledge and self-care practices regarding diabetes among newly diagnosed type 2 diabetics in Bangladesh: a cross sectional study. BMC Public Health. 2012;12:1112 [PubMed] | [CrossRef] | [Google Scholar]
- Khamseh ME, Vatankhah N, Baradaran HR. Knowledge and practice of foot care in Iranian people with type 2 diabetes. Int Wound J. 2007;4(4):298-302. [PubMed] | [CrossRef] | [Google Scholar]
- Mazzuca SA, Moorman NH, Wheeler ML, Norton JA, Fineberg NS, Vinicor F, et al. The diabetes education study: a controlled trial of the effects of diabetes patient education. Diabetes Care. 1986;9(1):1-10. [PubMed] | [CrossRef] | [Google Scholar]
- Balagopal P, Kamalamma N, Patel TG, Misra R. A community-based diabetes prevention andmanagement education program in a rural village in India. Diabetes Care. 2008;31(6):1097-104. [PubMed] | [CrossRef] | [Google Scholar]
- Otero LM, Zanetti ML, Ogrizio MD. Knowledge of diabetic patients about their disease before and after implementing a diabetes education program. Rev Lat Am Enfermagem. 2008;16(2):231-7. [PubMed] | [CrossRef] | [Google Scholar]