ABSTRACT
Introduction
Musculoskeletal disorders are injuries or illnesses that affect the muscles, nerves, tendons, joints, cartilage, and spinal discs. These disorders are characterized by a loss of physical function in the body as well as discomfort and pain, which limits a person’s activities and restricts their participation in society. Severe and long-term musculoskeletal disorders can have negative impact on quality of life, reduces work productivity, increases work absenteeism, shorten working life, and creates chronic occupational incapacity. All of which are serious health concerns for individuals and healthcare systems worldwide.
Objectives
This study was aimed at determining the prevalence of musculoskeletal disorders and health-related quality of life in patients who visited secondary healthcare settings. And, to analyse the socio-demographic characteristics of the study population with musculoskeletal disorders, and to evaluate the impact of musculoskeletal disorders on health-related quality of life.
Materials and Methods
An observational study of six months duration was carried out at a secondary care referral hospital. EuroQol EQ-5D-5L and EQ-VAS tools are used in the assessment of health-related quality of life and self-reported health status.
Results and Conclusion
The prevalence of musculoskeletal disorders was 11.95% among study participants. Through the health-related quality of life, it was found that the majority of the participants were facing slight to severe problems as defined by five dimensions.
INTRODUCTION
Musculoskeletal Disorders (MSDs) span a range of ailments affecting both hard and soft tissues of the musculoskeletal systems, including bones, joints and tendons, ligaments, cartilage, muscles, and nerves.1–3 These ailments are typically characterized by pain (often persistent) and limitations in mobility and dexterity, reducing people’s ability to work and participate in society. Pain experienced in musculoskeletal structures is the most common form of non-cancer pain. The World Health Organization (WHO) estimates that globally, approximately
1.71 billion people have had musculoskeletal conditions and the prevalence of musculoskeletal conditions varies by age and diagnosis. Approximately 441 million people in developed countries, 427 million people in the WHO western Pacific region, and 369 million people in the South–East region suffered from musculoskeletal disorders.4
Musculoskeletal disorders are the greatest contributors to Years Lived with Disability (YLDS) globally, accounting for around 149 million YLDS, or 17% of all years lived with disability.5 China is first in terms of years spent disabled, followed by India and the United States.6 According to the WHO, 40% of people over the age of 60 have musculoskeletal disorders, and about 80% of people have experienced low back pain at some point in their lives.7 Lower back pain plays a major role in the overall burden of musculoskeletal disorders, others include fractures, osteoarthritis, neck pain, rheumatoid arthritis and amputations.8
In India, the prevalence of musculoskeletal disorder varies widely. Epidemiological studies in various states showed a community-based prevalence of around 20% and an occupation-specific prevalence of up to 90%.9 The Indian Council for Medical Research (ICMR) estimated the prevalence in three northern states to be between 7.08 and 11.5 percent.10 In India, community survey data from rural and urban areas revealed a prevalence of osteoarthritis varied from 17% to 60%.11,12 Musculoskeletal pain was the most common self-reported ailment in the community, according to a WHO-LAR COPCORD (World Health Organization-International League of Associations for Rheumatology Community-Oriented Program for Control of Rheumatic Diseases) study conducted in Bigwig (1996-2014) near Pune.13 In Lucknow, a three-year study using the COPCORD model exhibited a strong prevalence of knee osteoarthritis, backache, and fibromyalgia.14 Another COPCORD study on musculoskeletal pain in Kerala found that the prevalence was 26.08 percent, with 8% of those affected needing to discontinue working and 4% suffering from serious depression.15 Other studies have also found that many of these illnesses occur more frequently in women.16–19
Women are more prone to MSDs than men for physiological and socioeconomic reasons.7,20,21 In supporting this Global Burden of Diseases-GBD 2017 estimates, women in India lost 35.8 percent greater Disability Adjusted Life Years (DALYs) per 100,000 than males in 2017.22 MSD was the major cause of work-related illness, accounting for about 33.8 percent of all new work-related musculoskeletal illnesses and nearly 77 percent in construction workers.23,24 According to global burden of disease data, India has moved to first place from second place in 2007 when it comes to aggregate DALYs lost, and now it has the largest number in the primary productive age range of 15-49 years. Within Asia, DALYs per 100,000 related to MSD are quite similar in India and Malaysia, Cambodia, and Indonesia. However, India exceeds other countries globally in terms of aggregate DALYs across all ages, ranking in second after China. In terms of DALYs per 100,000, in India, Uttar Pradesh has the highest number of DALYs lost related to MSD, followed by Maharashtra. In terms of DALYs lost per 100,000, Goa ranks high, followed by Kerala and Punjab.22 Long-term and severe MSDs can decrease quality of life, increase job absenteeism, shorten working lives, and cause chronic occupational disability, they are a major health challenge for individuals and healthcare systems all over the world.7,25,26
Musculoskeletal problems are also the leading cause of global rehabilitation needs. They account for over two-thirds of all adults in need of rehabilitation, and they are one of the major contributors to the demand for rehabilitation services among children.27 MSDs are the most prevalent cause of severe long-term pain and morbidity, affecting patient health and quality of life significantly, and placing a big economic burden on the healthcare system.10,28,29
Health aspects are often addressed and measured by Health-Related Quality of Life (HRQoL) questionnaires, such as the EuroQol five-dimensional questionnaire (EQ-5D), the Short Form 36 health survey questionnaire 12 and the Assessment of Quality of Life (AQoL) etc., Although numerous studies have reported on the quality of life of patients with musculoskeletal disorders across the globe, most of the research is focused on recording data on post-operative inflammation, mobility, muscle strength, range of motion, and factors contributing to disease progression but the data is limited in terms of evaluation of the clinical care to patients.
The current study was planned to assess, explore the prevalent risk factors and to identify its association with musculoskeletal conditions in secondary healthcare settings and to contribute for the existing prevalence of musculoskeletal conditions. Our study was planned to evaluate the subjective assessment of the health-related quality of life of patients with various musculoskeletal disorders at the orthopaedic department of secondary care referral hospital.
MATERIALS AND METHODS
Study design
The present study is a cross-sectional observational study.
Study site
The study was carried out at an outpatient orthopaedic department of a secondary care referral hospital.
Study Population
Patients attending orthopaedic department for their musculoskeletal complaints.
Study Criteria
Inclusion criteria
- The study included the following patient groups of both genders.
- Patients attending an orthopaedic unit who are over the age of 18 and of both genders.
- Patients newly diagnosed with musculoskeletal disorders.
- Patients with comorbidities and musculoskeletal disorders.
Exclusion criteria
- The following patient groups were excluded from the study.
- Patients attending the orthopaedic department aged below 18 years.
- Trauma fractures, accidental physical injury, or injury due to domestic violence occurred in all age groups and both genders.
- Patients who are not willing to participate in the study.
Study duration
The research was carried out over a six-month period.
Sample Size
The study enrolled 449 patients who met the inclusion criteria.
Study Tools
Participant data collection form
Data collection form includes demographics of participants, risk factors, past medical and medication history, current musculoskeletal complaints, diagnosis and associated comorbidities etc.
EuroQol Questionnaire30,31
EuroQol Questionnaire comprises of EQ-5D tool for assessment of health-related quality of life and EQ-VAS (visual analogue scale) to record health status.
EQ-5D is the most widely used preference-based multi-attribute health classification tool developed by the EuroQol Group, used to measure Health-Related Quality of Life (HRQoL) that can be presented as utility scores. It has two versions to measure HRQoL in adults: Five-dimensional three-level (EQ-5D-3L) and five-dimensional five-level (EQ-5D-5L) versions.
The EQ-5D-3L was introduced before the EQ-5D-5L, but they share the same five dimensions of mobility, self-care, usual activities, pain or discomfort and anxiety or depression.
The EQ-5D-3L has become the most widely-used Multi-Attribute Utility Instrument (MAUI) globally. However, concerns have arisen over the poor sensitivity and ceiling effects of the EQ-5D-3L. Therefore, the EQ-5D-5L was introduced in 2009. This comprises 3125 (55) health states and has a significantly reduced ceiling effect.
EQ-5D-5L descriptive systems five dimensions, five level responses were used in producing the utility scores (0 to 1) based on sub-population or country’s index scores (Indian 5-level version EQ-5D-5L value set) to place the respondents into 3,125 possible health states.
EQ-VAS is a vertical scale numbered from 0 (worst health) to 100 (best health) used to know how good or bad a participant’s health is today (i.e., on assessment day). For which each participant was asked to put ‘X’ mark on vertical scale and write the marked number in the provided box to depict their self-rated health status.
An approval to use this tool was obtained from EuroQol foundation.
Ethical Approval
The Institutional Review Board (IRB) approval was obtained (RIPER/IRB/PP/2021/007).
Study Procedure
The study participants were identified as per defined inclusion, exclusion criteria and explained the study protocol, procedure with clear objectives. Willingness to participate in the study was obtained through an informed consent form. The data from recruited participants was collected with a data collection form (demographics, risk factors, past medical and medication history, current complaints, diagnosis, comorbidities etc.,) followed by administration of EQ-5D-5L, EQ-VAS Health questionnaire in English and/or Telugu language (whichever is feasible for participants).
The obtained information was entered into Microsoft Excel 2019 and analyzed using GraphPad Prism 9.3.1. A student t-test with 95 percent confidence interval was performed to test for relationships, and p values of 0.05 were considered significant.
RESULTS
A total of 449 respondents agreed to participate in our study, with 116 (25.83%) male participants and 333 (74.16%) female participants. As per the inclusion criteria, the age distribution varies from 18 to 82 years. Table 1 presents the frequency distribution of the socio-demographic characteristics of the participants.
| Characteristics | Male (%) | Female (%) | Total (%) |
|---|---|---|---|
| Gender | 116 (25.84) | 333 (74.16) | 449 (100) |
| Age | |||
| 18-29 | 11 (2.45) | 14 (3.12) | 25 (5.57) |
| 30-39 | 6 (1.34) | 46 (10.24) | 52 (11.58) |
| 40-49 | 18 (4.01) | 87 (19.38) | 105 (23.39) |
| 50-59 | 45 (10.02) | 125 (27.84) | 170 (37.8) |
| 60-69 | 27 (6.01) | 54 (12.03) | 81 (18.04) |
| ≥70 | 9 (2.00) | 7 (1.56) | 16 (3.56) |
| BMI | |||
| Under Weight (<18.5) | 9 (2.00) | 14 (3.12) | 23 (5.12) |
| Normal Weight (18.5-24.9) | 84 (18.71) | 191 (42.54) | 275 (61.25) |
| Pre-Obesity (25.0-29.9) | 20 (4.45) | 97 (21.60) | 117 (26.06) |
| Obesity Class I (30.0-34.9) | 3 (0.67) | 23 (5.12) | 26 (5.79) |
| Obesity Class II (35.0-39.9) | 0 (00) | 2 (0.45) | 2 (0.45) |
| Obesity Class III (Above 40) | 0 (00) | 6 (1.34) | 6 (1.34) |
| Residence | |||
| Rural | 108 (24.05) | 308 (68.60) | 416 (92.65) |
| Urban | 8 (1.78) | 25 (5.57) | 33 (7.35) |
| Marital status | |||
| Married | 110 (24.50) | 323 (71.94) | 433 (96.44) |
| Unmarried | 6 (1.34) | 4 (0.89) | 10 (2.23) |
| Widowed | 0 (00) | 6 (1.34) | 6 (1.34) |
| Educational status | |||
| Illiterate | 36 (8.02) | 220 (49.00) | 256 (57.02) |
| Primary | 18 (4.01) | 37 (8.24) | 55 (12.25) |
| Middle | 22 (4.90) | 29 (6.46) | 51 (11.36) |
| Secondary | 34 (7.57) | 40 (8.91) | 74 (16.48) |
| Graduate | 6 (1.34) | 7 (1.56) | 13 (2.90) |
| Nature of work | |||
| Light | 14 (3.12) | 88 (19.60) | 102 (22.72) |
| Moderate | 24 (5.35) | 127 (28.29) | 151 (33.63) |
| Heavy | 78 (17.37) | 118 (26.28) | 196 (43.65) |
| Substance abuse | |||
| Yes | 36 (8.02) | 25 (5.57) | 61 (13.59) |
| No | 80 (17.82) | 308 (68.60) | 388 (86.41) |
From the age group analysis, it was found that the majority of patients belong to the 50-59 age group (170, 37.8%) followed by 40-49 (105, 23.39%), and 60-69 (81, 18.04%) age groups. When compared to the other age groups, the number of people aged 70 and above was very low. By virtue of a high female sample, female participants were high in all age groups except 70 and above.The majority of participants (275, 61.65%) fit into the normal-weight group according to the World Health Organization’s (WHO) Body Mass Index (BMI) classification, followed by pre-obesity (117, 26.06%), obesity class-I (26, 5.79%), and underweight (23, 5.12%). Since the study was conducted in rural settings, the majority of the respondents were solely from rural areas (416, 92.65%).
In this study, more than half of the participants were classified as illiterate (256, 57.02%), followed by secondary (74, 16.48%), primary (55, 12.25%), middle school (51, 11.36%), and graduate (13, 2.90%). Heavy work (196, 43.65%), moderate work (151, 33.63%), and light work (102, 22.72%) were reported by participants. Only 61 people, or 13.59% of those surveyed, said they had ever used drugs; the vast majority said no.
From Table 2 majority of participants (417, 92.87%) in the study of musculoskeletal complaints reported joint and/or muscle symptoms such swelling, soreness, stiffness, etc., whereas the remaining participants complained of back or spinal pain (177, 39.42%). The participants’ self-reported levels of physical activity ranged from low (130, 28.95%) to high (212, 47.22%) (107, 23.93%). The individuals’ self-rated levels of physical activity were moderate (212, 47.22%), low (130, 28.95%), and high (107, 23.93%). When questioned about absences from work owing to musculoskeletal symptoms, over half of the participants (190, 42.32%) claimed being absent for more than one month, followed by less than one week (79, 17.59%), and one week to one month (29, 6.46%) for their daily tasks. And 33.63 percent reported no or minimal absence from work.
| Characteristics | Male (%) | Female (%) | Total (%) |
|---|---|---|---|
| Musculoskeletal symptoms | |||
| Joint and/or Muscle symptoms | 107 (23.83) | 310 (69.04) | 417 (92.87) |
| Spine or back pain | 47 (10.47) | 130 (28.95) | 177 (39.42) |
| Physical activity level | |||
| Low | 24 (5.35) | 106 (23.61) | 130 (28.95) |
| Moderate | 42 (9.35) | 170 (37.86) | 212 (47.22) |
| High | 50 (11.14) | 57 (12.69) | 107 (23.83) |
| Absence of work | |||
| Nil | 30 (6.68) | 121(26.95) | 151 (33.63) |
| <1 week | 16 (3.56) | 63 (14.03) | 79 (17.59) |
| 1 week-1 month | 8 (1.78) | 21 (4.68) | 29 (6.46) |
| >1 month | 62 (13.81) | 128 (28.51) | 190 (42.32) |
| Functional status | |||
| No Limitations | 36 (8.02) | 64 (14.25) | 100 (22.27) |
| Limitations | 65 (14.48) | 236 (52.56) | 301 (67.04) |
| Restricted ambulation | 15 (3.34) | 33 (7.35) | 48 (10.69) |
| Co-morbidities | |||
| Yes | 18 (4.01) | 61 (14.03) | 79 (18.04) |
| No | 98 (21.83) | 272 (60.13) | 370 (81.96) |
In support of this, a few participants reported no limitations in functional status (100, 22.27%). While the majority reported limitations in daily activities, housework, and office work (301, 67.04%), only a few stated restrictions on ambulation (48, 10.69%). Participants’ medical histories reveal co-morbidities such as hypertension, diabetes, and hypo- and hyperthyroidism (81, 18.04%).
According to Figure 1, spondylitis was the most common (40.31%), followed by rheumatoid arthritis (31.18%), and osteoarthritis (28.51%) among study participants.
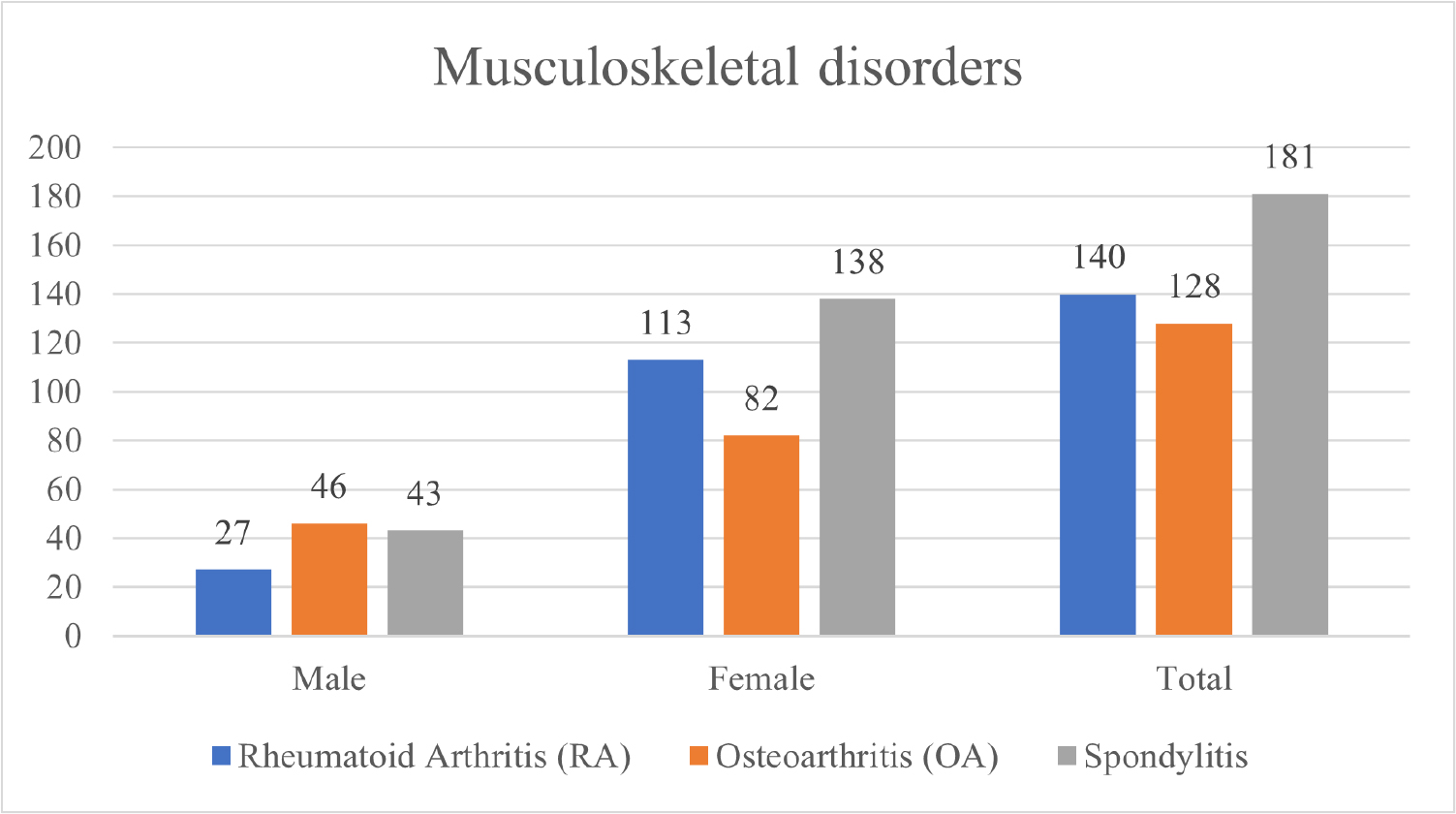
Figure 1:
Distribution of musculoskeletal disorders.
Table 3 presents the prevalence of musculoskeletal disorders, viz., rheumatoid arthritis (3.73%), osteoarthritis (3.41%), and spondylitis (4.81%). The overall prevalence of included musculoskeletal disorders was 11.96% among the study participants.
| Musculoskeletal disorder | Prevalence | ||
|---|---|---|---|
| Male | Female | Total | |
| Rheumatoid arthritis | 0.72% | 3.01% | 3.73% |
| Osteoarthritis | 1.22% | 2.18% | 3.41% |
| Spondylitis | 1.14% | 3.67% | 4.81% |
| Total Prevalence | 3.09% | 8.87% | 11.96% |
Figure 2 shows responses to questions about health-related quality of life obtained using the EQ-5D-5L descriptive system. An average of 7.06% of participants reported no problems, while the remaining participants reported minor to severe issues in the system’s five dimensions. All participants across the five parameters rated pain or discomfort as a minor to major issue.
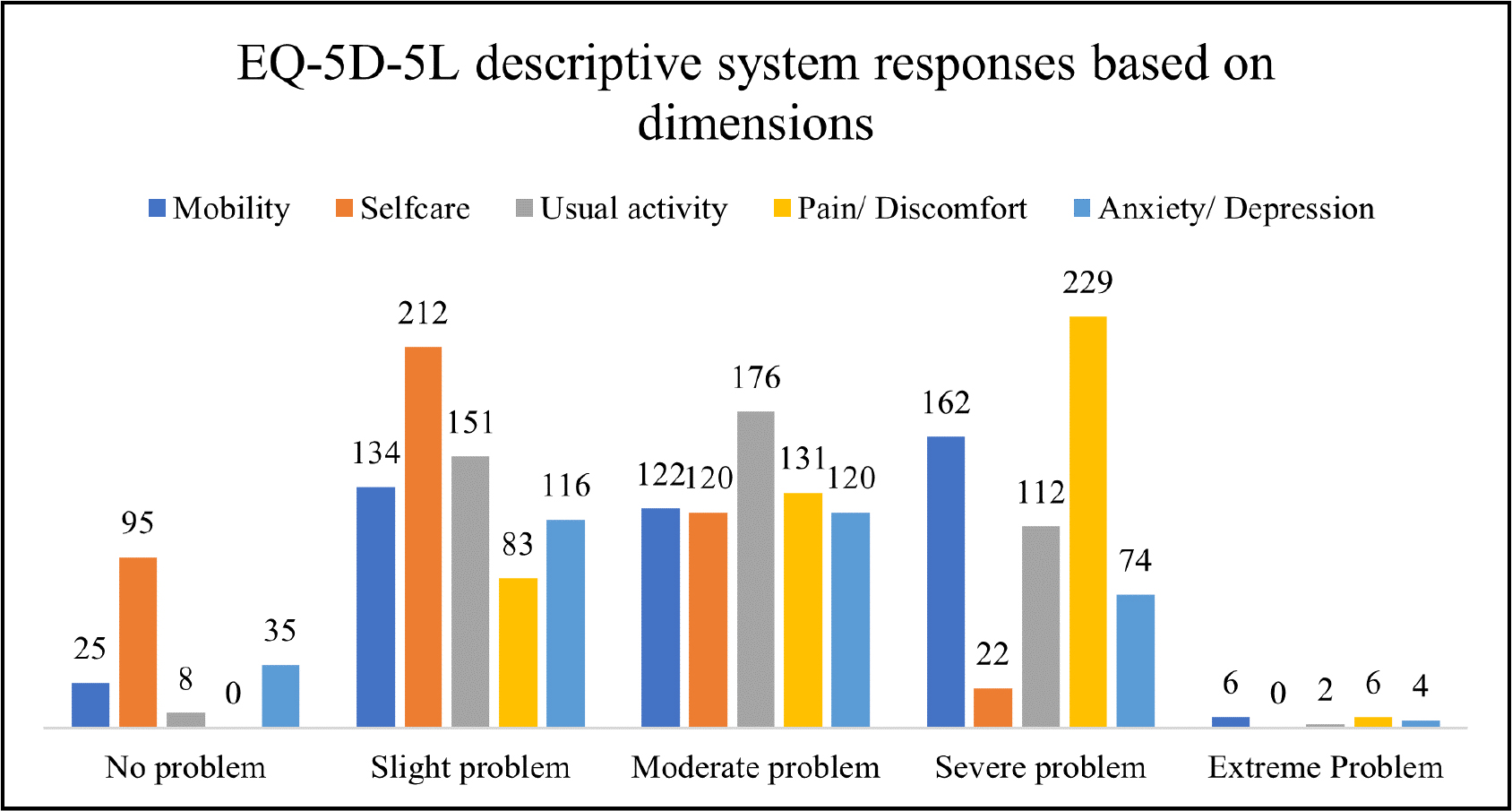
Figure 2:
EQ-5D-5L descriptive system responses based on dimensions.
Severe and slight problems were the most often mentioned level 4 and 2 responses in each dimension (i.e., 31% of responses from a total of 2,245), followed by moderate problems (level 3 response). And the least often mentioned response was “extreme problem” (level 5 response). About 5.57% of the participants had no problem with mobility, while 29.84%, 27.17%, 36.08%, and 1.34% had a slight, moderate, severe, and extreme problem with mobility; 21.16% of the participants had no problem with self-care, while 47.22%, 26.73%, 4.90% were had a slight, moderate, severe problem in self-care; 1.78% of the participants had no problem with usual activity, while 33.63%, 39.20%, 24.94%, 0.45% had a slight, moderate, severe, extreme problem with usual activity; 7.80% of the participants had no anxiety or depression, while 25.84%, 26.73%, 38.75%, 0.89% were had slight, moderate, severe, extreme anxiety or depression; 18.49%, 29.18%, 51.00%, 1.34% of the participants had slight, moderate, severe, extreme pain or discomfort respectively.
The mean of EQ-VAS self-rated health status was 58.82% on a 0–100 scale of worst to best health, which doesn’t enunciate either poor health or best health of the participants.
Table 4 shows participants mean Health-Related Quality of Life (HRQoL) utility scores by socio-demographic characteristics. The mean HRQoL utility score of the participants was 0.574. The average score for men was 0.563, while the average score for women was 0.579. EQ-5D-5L utility scores show significant differences in all groups of socio-demographic characteristics. The mean utility score for co-morbidities was a little low compared with the participants’ mean utility score. Among all the socio-demographic variants, the lowest utility score was observed in widowed women (0.462), and the highest utility score was observed in urban residents (0.641).
| Socio-demographic characteristics | Utility Score | |||
|---|---|---|---|---|
| N | Mean | SD | P Value |
|
| Gender | ||||
| Male | 116 | 0.563 | 0.1665 | 0.0089 |
| Female | 333 | 0.579 | 0.1834 | |
| Age | ||||
| 18-29 | 25 | 0.573 | 0.1354 | <0.0001 |
| 30-39 | 52 | 0.608 | 0.1719 | |
| 40-49 | 105 | 0.567 | 0.1915 | |
| 50-59 | 170 | 0.575 | 0.1865 | |
| 60-69 | 81 | 0.571 | 0.1662 | |
| ≥70 | 16 | 0.546 | 0.1775 | |
| BMI | ||||
| Under Weight (<18.5) | 23 | 0.544 | 0.1728 | <0.0001 |
| Normal Weight (18.5-24.9) | 275 | 0.593 | 0.1805 | |
| Pre-Obesity (25.0-29.9) | 117 | 0.558 | 0.1741 | |
| Obesity Class I (30.0-34.9) | 26 | 0.525 | 0.1964 | |
| Obesity Class II (35.0-39.9) | 2 | 0.565 | 0.0282 | |
| Obesity Class III (Above 40) | 6 | 0.587 | 0.1488 | |
| Residence | ||||
| Rural | 416 | 0.570 | 0.1766 | 0.0373 |
| Urban | 33 | 0.641 | 0.199 | |
| Marital status | ||||
| Married | 433 | 0.577 | 0.1795 | |
| Unmarried | 10 | 0.542 | 0.1347 | |
| Widowed | 6 | 0.462 | 0.2018 | |
| Educational status | ||||
| Illiterate | 256 | 0.573 | 0.1862 | <0.0001 |
| Primary | 55 | 0.609 | 0.1686 | |
| Middle | 51 | 0.523 | 0.181 | |
| Secondary | 74 | 0.596 | 0.1615 | |
| Graduate | 13 | 0.512 | 0.1324 | |
| Nature of work | ||||
| Light | 102 | 0.581 | 0.1966 | 0.0007 |
| Moderate | 151 | 0.602 | 0.1666 | |
| Heavy | 196 | 0.551 | 0.1765 | |
| Substance abuse | ||||
| Yes | 61 | 0.572 | 0.1919 | 0.0017 |
| No | 388 | 0.575 | 0.1773 | |
| Co-morbidities | 79 | 0.565 | 0.1800 | |
Figure 3 shows EQ-5D-5L mean utility scores corresponding to musculoskeletal disorders. The mean HRQoL utility score was low for rheumatoid arthritis (0.534), osteoarthritis (0.542), and spondylitis (0.628).
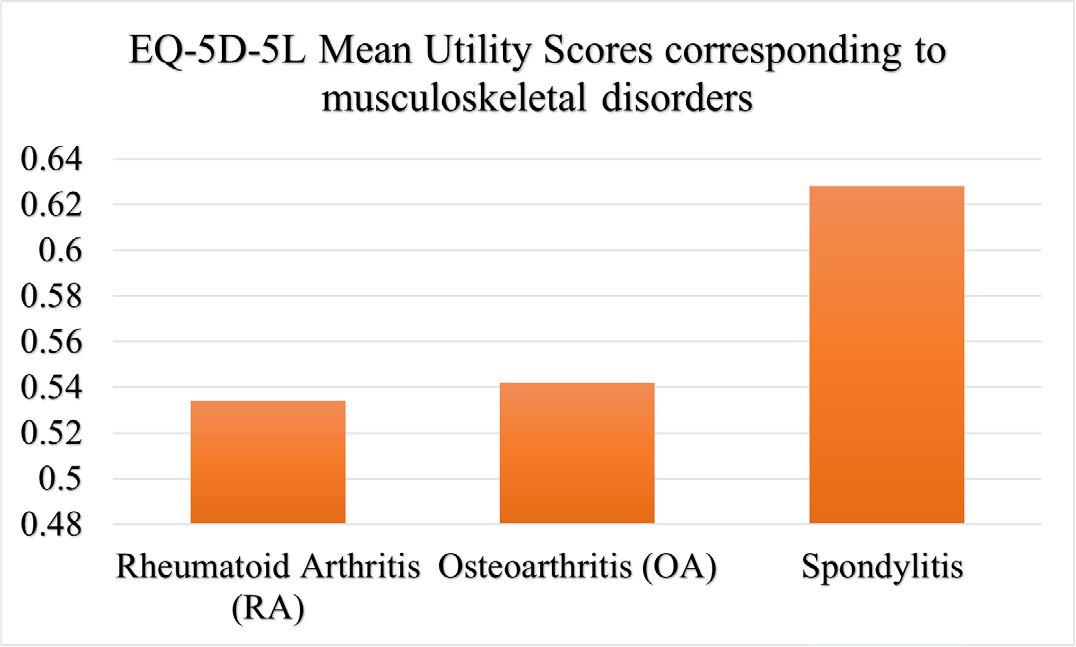
Figure 3:
EQ-5D-5L Mean Utility Scores corresponding to musculoskeletal disorders.
DISCUSSION
The aim of the study was to assess the health-related quality of life of patients with various musculoskeletal disorders presenting to the orthopaedic clinic, convert their responses into utility scores and explore the association between health-related quality of life and socio-demographic characteristics.
The prevalence of musculoskeletal disorders was 11.95%, which was similar to the prevalence estimated by the Indian Council for Medical Research (ICMR), 2012.10
In our study, the majority of the participants were female, with a 3:1 sex ratio. In terms of socio-demographic characteristics, the majority of the participants belong to the 50-59 age group, with a 1:2.7 male-to-female ratio. As obesity is one of the risk factors for musculoskeletal disorders, it was found that 117 (26%) participants belong to the pre-obesity category defined by the WHO. Since the study was conducted in rural settings, 92.6% of participants belong to a rural setup, and more than half of the participants (57%) were illiterate with poor substance abuse (86.4%).
Nearly half of the individuals (44%) missed more than a month of work due to underlying musculoskeletal disorders. And 77% of participants experienced difficulties performing basic functional tasks. The majority of the participants had lumbar spondylitis, which was followed by rheumatoid arthritis and osteoarthritis in terms of diagnosis.
The current study provided the EQ-5D-5L HRQoL utility scores, self-rated EQ-VAS health status, and their determinants among the patients visiting secondary healthcare settings. About 5.57%, 21.16%, 1.78%, 0%, and 7.80% of the participants reported no problem on mobility, self-care, usual activity, pain or discomfort, and anxiety or depression, respectively; 1.34%, 0%, 0.45%, 1.34%, and 0.89% of the participants reported extreme problem on mobility, self-care, usual activity, pain or discomfort, and anxiety or depression, respectively, while remaining participants reported a slight to severe level of problem for five dimensions.
The HRQoL mean utility score was 0.574 ± 0.179 based on index values calculated by using the EuroQol groups’ EQ-5D Index Value Calculator and Coefficients developed by the DEVINE valuation study.32 The EQ-VAS mean score was 58.82 ± 14.54. To our knowledge, no EQ-5D-5L HRQoL utility scores have been published for musculoskeletal disorder patients visiting secondary healthcare settings. However, Indian population EQ-5D-5L values set published by Prinja et al. in 2021.32 In their study, the overall mean utility score was 0.849 ± 0.212, mean EQ-VAS was 75.18 ± 16.41. And a Quebec population study by Poder et al. in 2019 states the overall mean utility score was 0.824.33 These results are clinically superior to those achieved in our research.
The HRQoL mean utility score (mean EQ-5D ± SD) for RA was 0.534 ± 0.181, which was lower than that of the Spanish population (0.63 ± 0.20),34 Korean population (0.70 ± 0.26),35 Danish population (0.73 ± 0.19),36 Japanese population (0.76 ± 0.18)37 and Thai patients (0.87 ± 0.13) with RA.38 And for ankylosing spondylitis patients, the HRQoL mean utility score (mean EQ-5D ± SD) was 0.628 ± 0.17, which was lower than the EQ-5D of Thai patients with ankylosing spondylitis (0.75 ± 0.2).38 EQ-5D-5L utility scores show significant differences in all groups of socio-demographic characteristics. These results were supported by similar findings by Poder et al. in 2019 and Grochtdreis T et al. in 2019.34,39
Although musculoskeletal disorders affect people of all ages and drive-up healthcare costs worldwide, much of the available literature focuses on a specific disorder, and very few attempts have been made to assess factors such as overall functionality, anxiety, self-rated health status, pain, and coping with daily activities in patients with acute or chronic musculoskeletal disorders. Despite their significant worldwide effect, these illnesses do not receive the attention they need because, unlike other fatal, non-communicable diseases, these disorders are seen to be less severe, non-fatal, and a result of ageing.
Furthermore, the scant availability of data in the country makes it indeed a daunting task to provide realistic estimates of the burden of MSDs. Considering the high prevalence of musculoskeletal disorders and economic burden, a better understanding of factors impacting HRQoL by using generic or specific questionnaires as a supplementary aid would help the healthcare professional in better understanding the patients’ health-related needs and improve their ability to manage these patients effectively.
CONCLUSION
The prevalence of musculoskeletal disorders was found to be 11.95% among study participants. Through EQ-5D-5L descriptive analysis, we found the majority of the participants were facing slight to severe problems, indicating poor quality of life, which was supported by a low health-related quality of life mean utility score of 0.574 and a mean EQ-VAS of 58.82.
References
- Dennerlein JT. Ergonomics/Musculoskeletal Issues. International Encyclopedia of Public Health. 2008:443-52.
- Giaccone M.. European Foundation for the Improvement of Living and Working Conditions, Managing Musculoskeletal Disorders [Internet]. 2007
- Villa-Forte A.. [2023 Mar 18];Introduction to symptoms of Musculoskeletal Disorders [Internet]. MSD Manual Consumer Version..
- [2023 Mar 18];Musculoskeletal health [Internet]. Who.int.. 2022
- Cieza A, Causey K, Kamenov K, Hanson SW, Chatterji S, Vos T., et al. Global estimates of the need for rehabilitation based on the Global Burden of Disease study 2019: a systematic analysis for the Global Burden of Disease Study 2019. Lancet. 2021;396(10267):2006-17. [Google Scholar]
- [2023 Mar 18];Global health estimates: Leading causes of DALYs [Internet]. Who.int.. [Google Scholar]
- Woolf AD, Pfleger B. Burden of major musculoskeletal conditions. Bull World Health Organ.. 2003;81(9):646-56. [Google Scholar]
- Cao B, Stevens G, Ho J, Ma D.. [2023 Mar 18];WHO methods and data sources for global burden of disease estimates. Who.int.. 2020 [Google Scholar]
- Yasobant S, Mohanty S.. Musculoskeletal disorders as a public health concern in India: A call for action. Physiotherapy. 2018;12(1):46 [Google Scholar]
- [Google Scholar]
- Sharma MK, Swami HM, Bhatia V, Verma A, Bhatia S, Kaur G, et al. An epidemiological study of correlates of osteoarthritis in the geriatric population of UT Chandigarh. Indian J Community Med. 2007;32:77-8. [Google Scholar]
- Kishore S, Garg BS. Sociomedical problems of aged population in a rural area of Wardha district. Indian J Public Health. 1997;41(2):43-8. [Google Scholar]
- Chopra A.. Disease burden of rheumatic diseases in India: COPCORD perspective. Indian J Rheumatol.. 2015;10(2):70-7. [Google Scholar]
- Kumar P, Alok R, Das SK, Srivastava R, Agarwal GG. Distribution of rheumatological diseases in rural and urban areas: An adapted COPCORD Stage I Phase III survey of Lucknow district in north India. Int J Rheum Dis. 2018;21(11):1894-9. [Google Scholar]
- Mathew AJ, Chopra A, Thekkemuriyil DV, George E, Goyal V, Nair JB, et al. Impact of musculoskeletal pain on physical function and health-related quality of life in a rural community 16 in South India: a WHO-ILAR-COPCORD-BJD India study. Clin Rheumatol. 2011;30(11):1491-7. [Google Scholar]
- Pingle AS, Pandit DD. A cross sectional study of Rheumatic Musculoskeletal Disorders (RMSDs) in an urban slum population. Indian J Community Med.. 2006:31.e5 [Google Scholar]
- Mahajan A, Jasrotia DS, Manhas AS, Jamwal SS. Prevalence of Major Rheumatic Disorders in Jammu. JK Sci Journal of Med Ed and Res. 2003;5(2):63-6. [Google Scholar]
- Venkatachalam J, Natesan M, Eswaran M, Johnson AKS, Bharath V, Singh Z, et al. Prevalence of osteoarthritis of knee joint among adult population in a rural area of Kanchipuram District, Tamil Nadu. Indian J Public Health.. 2018;62(2):117-22. [Google Scholar]
- Bihari V, Kesavachandran C, Pangtey BS, Srivastava AK, Mathur N. Musculoskeletal pain and its associated risk factors in residents of National Capital Region. Indian J Occup Environ Med.. 2011;15(2):59-63. [Google Scholar]
- Treaster Delia, Burr Deborah, Gorder Pam Frost. [2023 Mar 20];Women at least twice as likely to get some musculoskeletal disorders [Internet]. Women At Least Twice as Likely to Get Some Musculoskeletal Disorders. The Ohio State University. 2004 [Google Scholar]
- Côté J.. Can using a sex/gender lens provide new insights into MSD mechanisms?. 9th International Scientific Conference on the Prevention of Work-Related Musculoskeletal Disorders (PREMUS 2016) [Internet]. 2016 [Google Scholar]
- [Google Scholar]
- Reddy GMM, Nisha B, Prabhushankar TG, Vishwambhar V.. Musculoskeletal morbidity among construction workers: A cross-sectional community-based study. Indian J Occup Environ Med [Internet]. 2016;20(3):144-9. [Google Scholar]
- Punnett L, Wegman DH. Work-related musculoskeletal disorders: the epidemiologic evidence and the debate. J Electromyogr Kinesiol [Internet]. 2004;14(1):13-23. [Google Scholar]
- Vos T, Flaxman AD, Naghavi M, Lozano R, Michaud C, Ezzati M, et al. Years Lived with Disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990-2010: a systematic analysis for the global burden of disease study 2010. Lancet. 2010;380(9859):2163-96. [Google Scholar]
- Hagen K, Linde M, Heuch I, Stovner LJ, Zwart J-A. Increasing prevalence of chronic musculoskeletal complaints. A large 11-year follow-up in the general population (HUNT 2 and 3). Pain Med [Internet]. 2011;12(11):1657-66. [Google Scholar]
- [Google Scholar]
- Urwin M, Symmons D, Allison T, Brammah T, Busby H, Roxby M, et al. Estimating the burden of musculoskeletal disorders in the community: the comparative prevalence of symptoms at different anatomical sites, and the relation to social deprivation. Ann Rheum Dis [Internet]. 1998;57(11):649-55. [Google Scholar]
- Tüzün EH. Quality of life in chronic musculoskeletal pain. Best Pract Res Clin Rheumatol [Internet].. 2007;21(3):567-79. [Google Scholar]
- EuroQol-a new facility for the measurement of health-related quality of life. Health Policy.. 1990;16(3):199-208. [Google Scholar]
- . EuroQol: the current state of play. Health Policy [Internet]. 1996;37(1):53-72. [Google Scholar]
- Jyani G, Sharma A, Prinja S, Kar SS, Trivedi M, Patro BK, et al. Development of an EQ-5D Value set for India using an Extended design (DEVINE) study: The Indian 5-level version EQ-5D value set. Value Health [Internet]. 2022;25(7):1218-26. [Google Scholar]
- Poder TG, Carrier N, Kouakou CRC. Quebec health-related quality-of-life population norms using the EQ-5D-5L: Decomposition by sociodemographic data and health problems. Value Health [Internet]. 2020;23(2):251-9. [Google Scholar]
- Carreño A, Fernández I, Badia X, Varela C, Roset M.. Using HAQ-DI to estimate HUI-3 and EQ-5D utility values for patients with rheumatoid arthritis in Spain. Value Health [Internet]. 2011;14(1):192-200. [Google Scholar]
- Kim H-L, Kim D, Jang EJ, Lee M-Y, Song HJ, Park S-Y, et al. Mapping Health Assessment Questionnaire Disability Index (HAQ-DI) score, pain Visual Analog Scale (VAS), and Disease Activity score in 28 joints (DAS28) onto the EuroQol-5D (EQ-5D) utility score with the KORean Observational study Network for Arthritis (KORONA) registry data. Rheumatol Int [Internet]. 2016;36(4):505-13. [Google Scholar]
- Linde L, Sørensen J, Østergaard M, Hørslev-Petersen K, Hetland ML. Does clinical remission lead to normalization of EQ-5D in patients with rheumatoid arthritis and is selection of remission criteria important?. J Rheumatol [Internet]. 2010;37(2):285-90. [Google Scholar]
- Hoshi D, Tanaka E, Igarashi A, Inoue E, Kobayashi A, Sugimoto N, et al. Profiles of EQ-5D utility scores in the daily practice of Japanese patients with rheumatoid arthritis; Analysis of the IORRA database. Mod Rheumatol [Internet]. 2016;26(1):40-5. [Google Scholar]
- Wanruchada K, Pongthorn N, Wanwisa C, Phakhamon T.. Health-related quality of life in patients with rheumatoid arthritis. BMC Rheumatology. 2019;3:34-41. [Google Scholar]
- Grochtdreis T, Dams J, Konig HH, Konnopk A.. Health-related quality of life measured with the EQ-5D-5L: estimation of normative index values based on a representative German population sample and value set. Eur J Health Econ [Internet]. 2019;20(6):933-44. [Google Scholar]