ABSTRACT
Introduction
Antibiotics have important roles in human health, whereas irrational use of antibiotics is a major problem of public health that leads to resistance and ADRs. This study aimed to evaluate the prescribing pattern along with adverse drug reactions of antibiotics.
Materials and Methods
A hospital-based prospective observational study was conducted on 960 patients from September 2021 to February 2022. All of the treatment charts were used to review for prescribed patterns of antibiotic drugs in infected patients, when required data were found processed and noted in performed data form. This data were included antibiotics ADRs, patients’ personal information and Antibiotics prescribed pattern details. Patients were under monitoring and followed up till discharged or shifted to other wards.
Results
56.87% were male and most ages were above 51. Diabetes mellitus and respiratory diseases were the most common diseases found among infected patients. The average of antibiotics used per patient was 2.09. Penicillins were the most prescribed antibiotics among patients and they were used mostly for prophylaxis and treatment of infection diseases and respiratory diseases. 25.62% of patients found with antibiotics ADRs (9.37% males, 16.25% females); Most of the ADRs belonged to penicillins (31.76%) and carbapenems (17.64%) and most organs affected by ADRs were GIT, skin and muscles; based on severity and causality 60% were moderate and 63.52% were probable.
Conclusion
Antibiotics in high numbers and different classes were used and caused ADRs on patients to a lesser extent that indicates good quality of prescribing policies and requirements in process of the hospital.
INTRODUCTION
Antibiotics use to treat of infectious diseases by bacteria. Antibiotics have different and important roles in human health and life, which can be affected and affiliated by them; whereas irrational use of antibiotics is the major problem of public health that leads to antibiotic resistance and Adverse Drug Reactions (ADRs).1–4 Now, question is that the antibiotics have a long and important role in the health of humanity, is their use with awareness and is beneficial to human’s conditions yet.
In one study in America (2007-09), antibiotics were prescribed for adults during 95 million office visits per year and compared to European countries while the rate of antibiotic use in USA was higher, in other hands this study explained that the antibiotics were prescribed for viral infections that did not benefit and it could indicate antimicrobial resistance behind overuse of antibiotics and lead to harmful adverse events;5 but with the passage of time and variety of studies in this area, it would have increased the knowledge about the use of antibiotics. There are different reasons for Antibiotics like classifications, type of antibiotics, doses and dosage forms of antibiotics and also other conditions like co-morbidity and morbidity, age, gender and weight of patients can be effective on antibiotic choice at different conditions6 and even other situations related to hospitals, countries, races and health politicians have taken some special consumption pattern of antibiotics. In this regard prescribing pattern of antibiotics needs to be evaluated in any particular area they are used.7–9 Generally studies conducted about antibiotics in a different part of the world have usually reported that penecillins, cephalospirins, and fluroquinolons were the most prescribed class of antibiotics,10 but in few of the studies, macrolides were among the most antibiotics prescribed.11–13
An adverse drug reaction is an unwanted response by the human body to a drug which is used for a specific aim of treatment; World Health Organization (WHO) defined ADRs as any response to a drug which occurs at doses normally used in men for prophylaxis, diagnosis or therapy of diseases and the Food and Drug Administration (FDA) defined ADRs as an event that in different classes related to drug or device or by which the patient outcome is death or put the life treating at a real risk of dying.10,14,15 Adverse drug reactions are considered one of the leading causes of morbidity and mortality.15 Approximately 10-20% of hospital inpatients had an experience adverse drug reactions and up to 7% of hospital admissions are directly due to adverse drug reactions; among the drugs caused adverse drug reactions antibiotics were the most frequency caused ADRs and followed by the anti-tremors.16 In the other hand unwanted effects of drugs are more common in elderly patients which can be related to polypharmacy prescribing, their co-morbidity and physical variables.
By following the various uses of antibiotics under different conditions and the polypharmacy with antibiotics, many adverse effects were reported that kept human’s life in a particular stage, these results were in similar form about adverse effects in all of those studies, with approximately the highest rate of these side effects reported in antibiotic studies was related to GIT and muscles and skin damages. This study considered to aim and evaluate the prescribing pattern and adverse drug reactions of antibiotics in inpatient wards of a tertiary care hospital. In addition, this study can produce evidence for healthcare systems to enhance and establish understanding importance of antibiotics and their prescriptions or confirm the findings of previous studies on antibiotics.
MATERIALS AND METHODS
A hospital-based prospective observational study was conducted on 960 patients for a period of 6 months from September 2021 to February 2022 in wards/departments of Bangalore Baptist Hospital (BBH), Bengaluru. All of the Prescribed and treatment charts of inpatients used to review for prescribed patterns and evaluation ADRs of antibiotic drugs in case of infected patients. References, articles, software, scales and books are used as tools to review the prescribed antibiotics and cases (patients) charts.
Previous studies on antibiotics used in infected patients were conducted at hospitals on the large number of patients for periods from six months to more than one year; these studies used forms and tools like a specified data collection form including patients information, a drug user and lab parameters that were important in studies,17,18 Hartwig scale for evaluation of severity, naranjo or WHO scales for evaluation of ADRs causality,14 Rawlin and Thomson used for classification of ADRs based on their type.11 Beside these forms software like Medscape, up-to-date and Micromedex were used to help in the evaluation of ADRs.19,20
All medically relevant information was noted in a predefined Data Collection Form (DCF). Alternatively, DCF was an important part of the study, which contained demographic data and the detailed history of the patient that was regarding past, family, personal and drug history use (especially antibiotics).
Other details for hospitalization like the present diagnosis, reason for admission, Antibiotic prescribed details (dosage forms, doses, frequency, route and days of use) and related antibiotics adverse drug reactions also noted if they were found.
A professional form was prepared with all of the details about ADRs to study the antibiotics prescribed during hospitalization; in this form for the evaluation of probability and causality of antibiotics ADRs the NARANJO scale was the choice because of its available and well known, also for the severity of antibiotics adverse drug reactions Hartwig scale was used. Besides these scales Medscape and Micromedex and a face scale were used to evaluate adverse drug reactions. Alternatively, it was on this agreement and idea that to find those patients who stayed for more than three days at wards to get better evidence of ADRs.
Patients of both genders who were admitted into the inpatient wards of the hospital and patients in age greater than 18 years were included in this study. It was considered to exclude patients from pediatric wards, pregnant women and patients from Out Patient (OP) departments, because of the different and difficult process needed to evaluate antibiotics among them or because of complications of study that could take a long time to cross over of a complete study.
According to the above details, patients were evaluated for the first time to enter the study, their information was recorded into DCF, and followed up daily by checkout the medication chart, nurses and physicians reports, lab parameters reports and patient’s self-report of new or progressive abnormalities during hospitalization. This follows up was continued till the patients were discharged or shifted to other wards; when data collection was finished they were entered to windows Excel and used for the last evaluation.
Statical Analysis
Descriptive statistics were applied for the calculation of mean, standard deviation, frequencies, and percentage of patient’s demographic/clinical characteristics, and medication-related data. The statistical package for social sciences for windows, version 22.0 was used for data analysis.
RESULTS
The present study identified the prescribing pattern and ADRs conducted among the antibiotics used for 960 patients admitted to the different wards of a hospital. According to the gender of patients, 56.87% of patients were male and 43.12% were female; these distributions of patients based on the genders are displayed in Table 1. Based on the age most of the patients were in ages of 51 to 70 years (44.37%) followed by patients with ages higher than 70 years old (geriatric) (35%), distribution of patients based on age is displayed in Table 1. Therefore, in this study, most of the patients were prescribed for antibiotics were in elderly ages and men was more than women.
| Parameters | No | % | |||
|---|---|---|---|---|---|
| Sex | |||||
| Male | 546 | 56.87% | |||
| Female | 414 | 43.12% | |||
| Age | |||||
| 18-30 | 78 | 8.12% | |||
| 31-50 | 120 | 12.5% | |||
| 51-70 | 426 | 44.37% | |||
| > 70 | 336 | 35% | |||
| Allergy | |||||
| Allergy To Antibiotic | 36 | 3.75% | |||
| Antibiotics History Use | |||||
| History Of Use | 570 | 59.37% | |||
| No History Of Use | 390 | 40.62% | |||
| Morbidities | |||||
| Past | Diagnosis | Past | Diagnosis | ||
| Nervous Diseases | 126 | 192 | 13.12% | 20% | |
| Heart And Vessels Diseases | 156 | 210 | 16.25% | 21.87% | |
| Respiratory | 306 | 864 | 31.87% | 50.62% | |
| Tract System Diseases | 444 | 282 | 46.25% | 29.37% | |
| Diabetes Mellitus | 282 | 336 | 29.37% | 35% | |
| Hypertension | 84 | – | 8.75% | – | |
| Hormonal | 72 | 174 | 7.5% | 18.12% | |
| Diseases | 66 | 36 | 11.87% | 3.75% | |
| Febrile Illness | 96 | 84 | 10% | 8.75% | |
| Accident Situations | 144 | 168 | 15% | 17.5% | |
| Gastrointestinal System Disease | 192 | 450 | 20% | 46.87% | |
| Urinary Tract Diseases | – | 126 | – | 13.12% | |
| Bacterial Infection Diseases | 132 | 156 | 13.75% | 3.75% | |
| Viral Infection Diseases | 54 | – | 5.6% | – | |
| Other Rare Situations | |||||
| Not Specified | |||||
Among these patients 46.25% had diabetes mellitus and followed by 31.87% with respiratory diseases as major co-morbidities; On the other hand, most of the patients were mainly diagnosed with bacterial infection diseases (46.87%) and followed by respiratory diseases (50.62%) when they were admitted to hospital and antibiotics prescribed for them; So, diabetes mellitus, bacterial infection diseases and respiratory diseases were the common conditions among patients prescribed for antibiotics. During the study 36 (3.75%) patients had reports of allergy to antibiotics, also according to the history of the antibiotics used before admission to the hospital, 59.37% of patients were identified with previous use of antibiotics and 40.62% had no history of antibiotic use; all of this details are displayed in Table 1.
Totally 2004 Antibiotics were prescribed to 960 patients during their treatment at a hospital, most of these antibiotics were penicillins and followed by cephalospirins and fluorquinolons, among this antibiotics Piperacillin/tazobactam (17.55%) was the most used antibiotic that in followed by Azithromycin (10.41%) and Ceftriaxone (9.52%) at a slight distance, the average of antibiotics used per patients were 2.09 antibiotics; the details of antibiotics distributions are displayed in Figures 1 and 2. Among these antibiotics 64.37% were in form of injection solutions, 25.74% were in form of tablets and 9.88% were in form of capsules (Table 2); also it was found that 18.12% of patients were prescribed one antibiotic and 81.87% of patients were prescribed more than one antibiotic at their hospitalization, which is presented in Table 2. Therefore penicillins, cephalospirins and fluorquinolons were the first line of choice for treatment of infectious diseases in hospitals and most of the patients received more than one antibiotic.
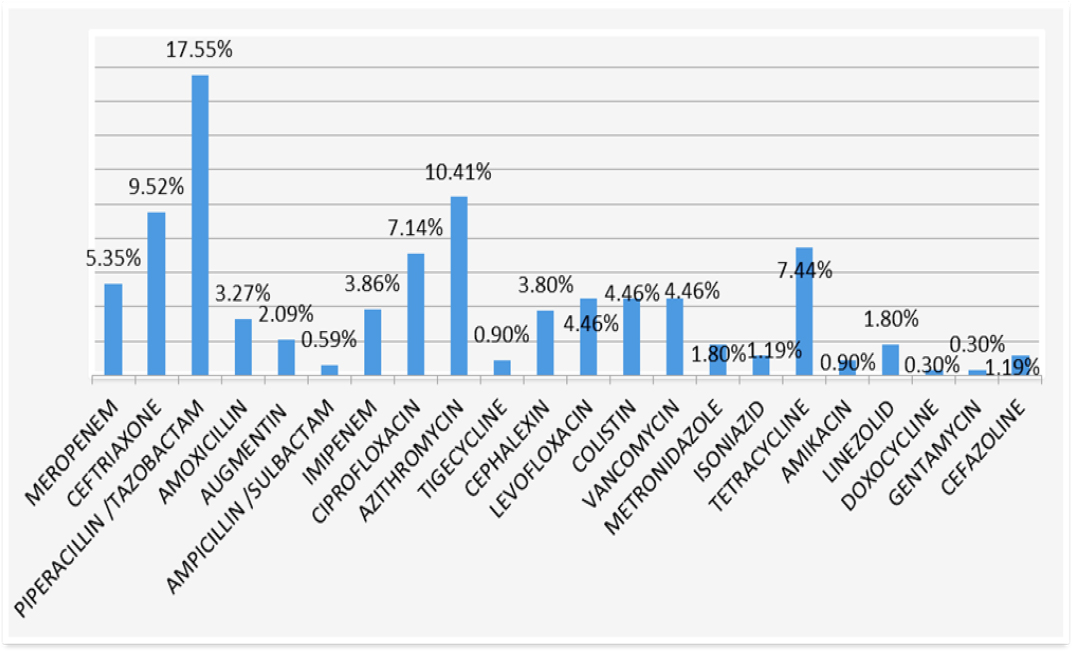
Figure 1:
Classification of antibiotics used.
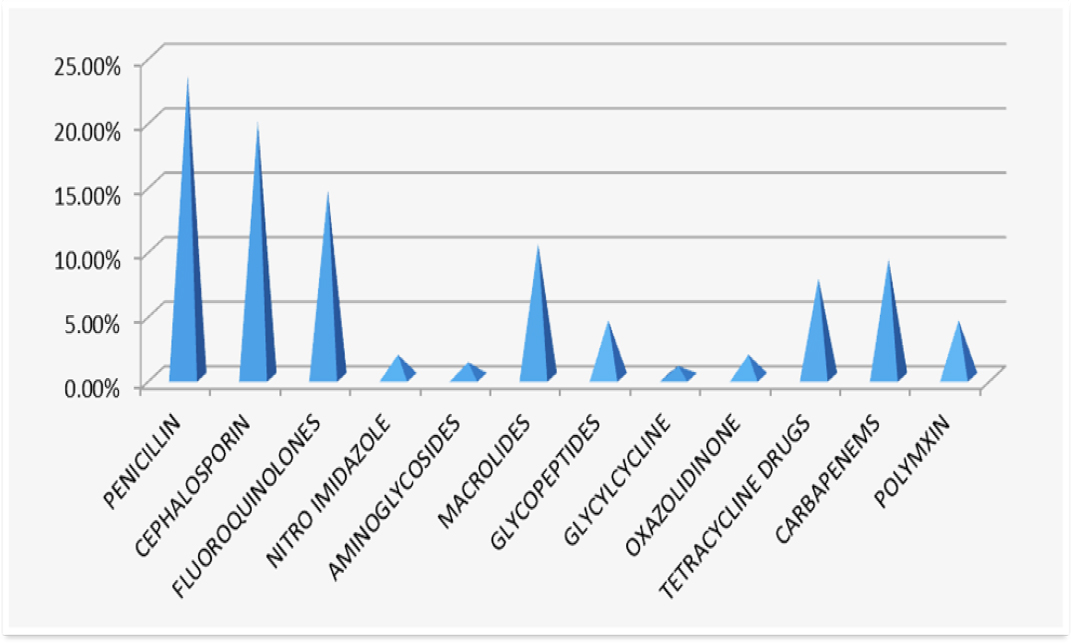
Figure 2:
The amount of antibiotic used.
| Titles | No | % |
|---|---|---|
| Dosage form of total antibiotics | ||
| Injection Solutions | 1290 | 64.37% |
| Tablet Form | 516 | 25.74% |
| Capsule Form | 198 | 9.88% |
| Antibiotic per patients | ||
| Monotherapy With Antibiotic | 174 | 18.12% |
| Multiple-Therapy With Antibiotic | 786 | 81.87% |
Adverse drug reactions of antibiotics which were the main point of the study were identified at 25.62% of patients, which in women (58.53%) more than in men (41.46%); on the other hand based on the number of antibiotics, 25.45% of them caused ADRs (Table 3). Most of the ADRs identified belong to penicillins (31.76% of total adverse effects) that followed by carbapenems (17.64% of total adverse effects) and cephalospirins (15.29%); The ADRs in relation to antibiotics class that was conducted in this study presented at Figure 3. According to this information conducted by study, a quarter of all antibiotics caused ADRs which were more in women.
| Details | No | % |
|---|---|---|
| Patient With ADRs | 246 | 25.62% |
| Drugs With ADRs | 510 | 25.45% |
| Male | 102 | 41.46% |
| Female | 144 | 58.53% |
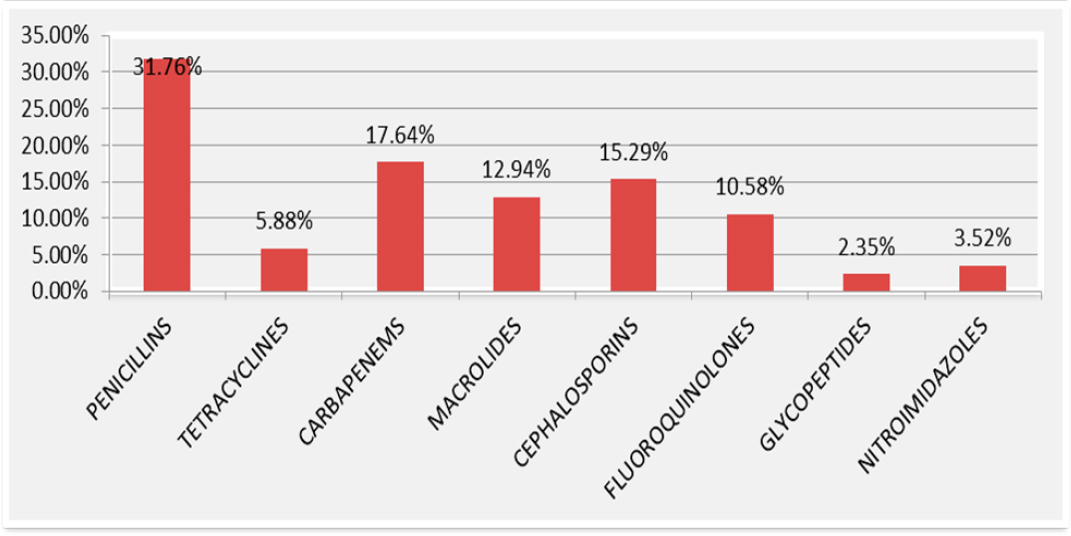
Figure 3:
Antibiotics caused ADRs.
By evaluation done on ADRs that which organs were more affected, the gastrointestinal tract (38.82%) and skin and muscles (25.88%) were the most affected organ while the lesser affected organs were respiratory and urinary as presented at Table 4. According to the severity of ADRs per Hartwig Scale 14.11% of adverse drug reactions were identified as severe, 60% were identified as moderate and 25.88% were mild, in other hands based on the per Naranjo scale 8.23% calculated as defined, 63.52% calculated as probable and 28.23% were possible; all of this details are displayed at Table 5. Therefore most of ADRs were moderate in severity and probable in causality assessment.
| Organs names | No of ADRs | % |
|---|---|---|
| Gastrointestinal Tract | 198 | 38.82% |
| Skin And Muscles | 132 | 25.88% |
| Blood And Heart | 60 | 11.76% |
| Nerve System | 18 | 3.53% |
| Urinary Tract System | 6 | 1.17% |
| Respiratory Tract System | 6 | 1.17% |
| Other
Different Organs |
90 | 17.64% |
| ADRs type | NO | % | |
|---|---|---|---|
| Severity | Severe | 72 | 14.11% |
| Moderate | 306 | 60% | |
| Mild | 132 | 25.88% | |
| Causality assessment | Defined | 42 | 8.23% |
| Probable | 324 | 63.52% | |
| Possible | 144 | 28.23% |
DISCUSSION
Antibiotics had an important role in humanity’s life; they are used for the treatment and prophylaxis of various infectious conditions and are considered safer drugs when used rationally. But, like all other drugs, they also show some adverse drug reactions in various patient conditions.14 Many studies have been conducted in this area but promoting information about the use of antibiotics and their possible ADRs can help to complement organizational risk management activities, assess the safety of drug therapies, measure ADR incidence rates over time, and educate health care professionals of drug effects and increase their level of awareness regarding ADRs.21 This study was considered to find out the prescribing pattern of antibiotics and evaluate the ADRs that were found during their use at a tertiary care hospital.
Two studies were conducted in Western Nepal9 and Kerala, India14 showed that the number of men receiving antibiotics was more than women and that a similar result was found in this study, therefore it can be clear that men are more prone to infectious diseases and receiving of the antibiotics compared to women. Based on the age at previous studies most of the patients who received antibiotics were in elderly age; studies like Ravi Pathiyil Shanks and et al. study showed 51.2% of patients were above the age of 59 years9 and other study conducted in an Indian dental centre showed that most of the patients received antibiotics were in the average age of 31.58+7.2 years,22 whereas in this study same result was obtained that most of patients were in ages of greater than 51 years old, This could be related to more incidences of infection diseases in the older population; in general, elderly patients are at higher risk for adverse effects because they are likely to have multiple diseases and polypharmacy that usually occur with an increased duration of disease conditions and altered physiology.
This study was observed that diabetes mellitus, respiratory diseases and infectious conditions were the most of situations that antibiotics prescribed for them; a similar result was reported in other studies conducted on infected patients, like a study in Singapore showed that diabetes and cardiac vascular system conditions were the most of situations22 and in a study at California Antibiotics were commonly prescribed for respiratory conditions.5 In general, diabetes mellitus, respiratory diseases along with infectious conditions were common in patients when they were admitted to hospital and antibiotics prescribed; co-morbidity increases the total burden of the illness in a patient and also contributes to clinical outcomes as well as to economic outcomes, adverse effects and other situations.
Totally 2004 number of antibiotics were prescribed for 960 patients, most of these antibiotics were penicillins and followed by cephalospirins and fluorquinolons, among this antibiotics Piperacillin/tazobactam was the most used antibiotic followed by Azithromycin and Ceftriaxone at a slightly distance; in Also by calculation in the information obtained in this study the average of antibiotics used per patient was 2.09 antibiotics. Whereas in M. Shamna and et al. study most of antibiotics were from the cephalospirins followed by quinolones and penicillins1 and in other studies, most commonly prescribed antibiotics were from quinolones (25% of antibiotics), macrolides (20%) and penicillins (12%).5 also in the study by Pathiyil Shankar and et al., conducted an average of 1.7 antibiotics per patients.9 so, in general, penicillins, cephalospirins and fluorquinolons were the first choices in a treat of infection conditions and more than one antibiotic were used per patient at hospitals. In this study, 3.75% of patients had allergy reports to antibiotics and 59.37% had a history of antibiotic use before being admitted to the hospital; here is mentioned that the statistics of allergy and history use of antibiotics in some patients were not properly mentioned or not found at all, or remained empty and unchanged without evaluation. By having in the hand of information on the history of antibiotic used especially allergies and information on antibiotics can be helpful in the choice of antibiotics and reduce conditions like morbidity and mortality, ADRs and cost effects.
In a study in Western Nepal the results showed that ADRs were in low ratio and in males were more than females,9 while in this study Adverse drug reactions of antibiotics were identified at 25.62% of patients, on the other hand, based on the number of antibiotics, 25.45% of them caused ADRs; which shows that the rate of ADRs by antibiotics was low in this hospital and in women were more than men; therefore that men were more exposed of antibiotic ADRs or women are unpredictable and can be affected by variables. Most of the ADRs are identified were belongs to penicilins followed by carbapenems and cephalospirins; a study carried out by Ravi Pathiyil Shankar et al. showed that cephalosporins were the most accounted antibiotic class caused ADRs followed by fluoroquinolones and penicillins or in other study conducted at ambulatory care in England penicillins and cephalosporins have been widely responsible in ADR rate3 or at other studies in North Korea penicillins and quinolones were the most frequent causes of ADRs;23 so by considering that those antibiotics have been used widely admittedly more adverse effects were found from them like penicillins had higher numbers of users and had higher rate of ADRs in this study and other, which figure out that the number adverse effects depended on the number of the antibiotics prescribed among patients.
By evaluating done on ADRs in this study which organs were more affected, gastrointestinal tract (38.82%) and skin and muscles (25.88%) were the most affected organ; it was similar to most other study’s results on antibiotics with insignificance differences.13,20 Like an Indian study most common organ system affected by ADRs was dermatological (47.44%) followed by gastrointestinal (39.28%),24 it was clear that skin, muscles and GIT were mostly influenced by the unwanted effects of antibiotics. According to the severity of ADRs per Hartwig scale most ADRs were moderate (60%) and in lesser amounts severe and mild; also based on the causality assessment per Naranjo scale most ADRs were classified as probable (63.52%) and in lesser possible and defined. In one study in Kerala, India the level of severity of adverse effects reported that most ADRs were moderate (63.26%) followed in lesser amounts mild and severe, also their report on the probability of ADRs showed that 71.42% of adverse effects were probable and 18.36% were possible and 10.20% of adverse effects were defined.14 One study at North India reported the causality assessment by Naranjo scale classified that 71.69% as probable and 28.31% as possible while no case accounted as definite.13 So based on the information observed most of ADRs related to antibiotics were moderate in severity and probable in causality assessment.
CONCLUSION
Antibiotics at high numbers and different classes were used among patients with different conditions, in the other hand antibiotics are used as the strongest and most sturdy tools for prophylaxis and against infection conditions; for this reason, their use and role in the daily human’s life are wide while antibiotics can cause unwanted adverse effects; this study along with other studies have shown that their benefits are still more than their losses. Antibiotics that caused adverse drug reactions among patients in our hospital were at the lesser extent which means all requirements and policy for the prescription of antibiotics, especially in monitoring and reporting about adverse drug reactions by health care professionals like nurses, physicians and pharmacists on antibiotics were good, that shows the process of hospital and their use of antibiotics were almost rational.
References
- Demoz GT, Kasahun GG, Hagazy K, Wolddu G, Wahdey S, Tadesse DB, et al. Prescribing pattern of antibiotics using WHO prescribing indicators among inpatients in Ethiopia: A need for antibiotic stewardship program. Infect Drug Resist.. 2020:2783-94. [Google Scholar]
- Hutchings MI, Truman AW, Wilkinson B. Antibiotics: past, present and future. Curr Opin Microbiol.. 2019;51:72-80. [CrossRef] | [Google Scholar]
- Gould K.. Antibiotics: from prehistory to the present day. J Antimicrob Chemother. 2016;71(3):572-5. [PubMed] | [CrossRef] | [Google Scholar]
- Yen P, Papin JA. History of antibiotic adaptation influences microbial evolutionary dynamics during subsequent treatment. PLOS Biol.. 2017;15(8):e2001586 [PubMed] | [CrossRef] | [Google Scholar]
- Shapiro DJ, Hicks LA, Pavia AT, Hersh AL. Antibiotic prescribing for adults in ambulatory care in the USA, 2007-09. J Antimicrob Chemother. 2014;69(1):234-40. [PubMed] | [CrossRef] | [Google Scholar]
- Steinman MA, Landefeld CS, Gonzales R.. Predictors of broad-spectrum antibiotic prescribing for acute respiratory tract infections in adult primary care. JAMA. 2003;289(6):719-25. [PubMed] | [CrossRef] | [Google Scholar]
- Baddoura LM, Dayerb MJ, Thornhill MH. Adverse drug reactions due to oral antibiotics prescribed in the community setting – England. Nfectious Dis. 2019:1-4. [PubMed] | [CrossRef] | [Google Scholar]
- Aminov RI. A brief history of the antibiotic era: lessons learned and challenges for the future. Front Microbiol.. 2010;1:134 [PubMed] | [CrossRef] | [Google Scholar]
- Shankar RP, Partha P, Shenoy NK, Easow JM, Brahmadathan KN. Prescribing patterns of antibiotics and sensitivity patterns of common microorganisms in the Internal Medicine ward of a teaching hospital in Western Nepal: a prospective study. Ann Clin Microbiol Antimicrob.. 2003;2(1):7 [PubMed] | [CrossRef] | [Google Scholar]
- Rani S, Sharma B. T, Kumar S, Saini R.. Antibiotics-related adverse drug reactions at a tertiary care hospital in North India. Int J Basic Clin Pharmacol. 2019;8(10):2288-93. [CrossRef] | [Google Scholar]
- Thornhill MH, Dayer MJ, Durkin MJ, Lockhart PB, Baddour LM. Risk of adverse reactions to oral antibiotics prescribed by dentists. Int Am Assoc. J Dent Res. 2019;98(10):1-7. [PubMed] | [CrossRef] | [Google Scholar]
- Sharif SI, Al-Shaqra M, Hajjar H, Shamout A, Wess L.. Patterns of drug prescribing in A hospital in Dubai, United Arab Emirates. Libyan J AOP. 2008;3(1):10-2. [CrossRef] | [Google Scholar]
- Mitsi G, Jelastopulu E, Basiaris H, Skoutelis A, Gogos C.. Patterns of antibiotic use among adults and parents in the community: A questionnaire-based survey in a Greek urban population. Int J Antimicrob Agents. 2005;25(5):439-43. [PubMed] | [CrossRef] | [Google Scholar]
- Shamna M, Dilip C, Ajmal M, Linu Mohan P, Shinu C, Jafer CP, et al. A prospective study on Adverse Drug Reactions of antibiotics in a tertiary care hospital. Saudi Pharm J. 2014;22(4):303-8. [PubMed] | [CrossRef] | [Google Scholar]
- Srinivasan R, Ramya G.. Adverse drug reaction-causality assessment. IJRPC. 2011;1(3):606-12. [PubMed] | [CrossRef] | [Google Scholar]
- NOVOTNÝ J, NOVOTNÝ M.. Adverse drug reactions to antibiotics and major antibiotic drug interactions. Gen Physiol Biophys. 1999;18:126-39. [PubMed] | [Google Scholar]
- Jansen JW, Linneman TW, Tan X, Moenster RP. Comparison of adverse drug reactions between patients treated with ceftaroline or ceftriaxone: A Single-Center, matched cohort study. Open Forum Infect Dis.. 2019;6(7):ofz279 [PubMed] | [CrossRef] | [Google Scholar]
- Hornik CP, Herring AH, Benjamin DK, Capparelli EV, Kearns GL. John van den Anker. adverse Events Associated with meropenem versus imipenem/cilastatin Therapy in a Large Retrospective Cohort of Hospitalized Infants. Pediatr infect dis j author [manuscript]. available in PMC 2014 July 01.1-12. [PubMed] | [CrossRef] | [Google Scholar]
- Ann L. rulappen, Danial Monica, Sulaiman Syed. S.. Evaluation of Reported adverse Drug Reactions in antibiotic Usage: A Retrospective Study from a Tertiary Care Hospital, Malaysia. Array. 2018;9:1-6. [PubMed] | [CrossRef] | [Google Scholar]
- Jung KJJ, Lee SJ, Jinnam K, Seong H, Wooyong J. Antibiotic-Related adverse Drug Reactions at a Tertiary Care Hospital in South Korea. Biomed Res Int Oung Id.. 2017(4304973):1-7. [PubMed] | [CrossRef] | [Google Scholar]
- Jose J, Rao PGM. Pattern of adverse drug reactions notified by spontaneous reporting in an Indian tertiary care teaching hospital. Pharmacol Res. 2006;54(3):226-33. [PubMed] | [CrossRef] | [Google Scholar]
- Garg AK, Agrawal N, Tewari RK, Kumar A, Chandra A.. Antibiotic prescription pattern among Indian oral healthcare providers: a cross-sectional survey. J Antimicrob Chemother. 2014;69(2):526-8. [PubMed] | [CrossRef] | [Google Scholar]
- Chan SL, Ang X, Sani LL, Ng HY, Winther MD, Liu JJ, et al. Prevalence and characteristics of adverse drug reactions at admission to hospital: a prospective observational study. Br J Clin Pharmacol. 2016;82(6):1636-46. [PubMed] | [CrossRef] | [Google Scholar]
- Richa Tandon VR, Sharma S, Khajuria V, Mahajan V, Gillani Z.. Adverse drug reactions profile of antimicrobials: A 3-year experience, from a tertiary care teaching hospital of India. Indian J Med Microbiol. 2015;33(3):393-400. [PubMed] | [CrossRef] | [Google Scholar]